If you have uterine fibroids and are considering treatment or if you’ve heard about uterine morcellation in the news, this article will help you understand the issue.
What are power morcellation devices?
A power morcellation device is a small surgical tool which cut tissue into smaller pieces. This allows organs or other tissues to be removed through smaller incisions, making surgery shorter and leaving smaller scars behind. The front end of a power morcellator has a spinning blade that cuts the tissue into tiny pieces (pulverizes it), and the back end is connected to a tube which sucks the tissue through the device (see image below).
Power morcellation devices were originally designed for removal of the uterus (or the womb), but are currently used for many different types of surgical procedures because they make it easier for a physician to perform surgery using smaller incisions.
What is the controversy about morcellation devices?
In 2012, two Harvard doctors had their lives tragically affected by these devices. Dr. Amy Reed, an anesthesiologist at Beth Israel Deaconess Medical Center, which is affiliated with Harvard Medical School, had surgery in the fall of 2013 to remove her uterus due to fibroids. After the surgery she was diagnosed with advanced (stage IV) uterine cancer, spread by the use of power morcellation during her surgery. The morcellation left behind tiny pieces of tumor throughout her pelvic cavity, which allowed the cancer to spread. While morcellation devices are sometimes used with a bag to contain the fibroid or tissue so that it won’t spread, the bags can be difficult to use so not all surgeons use them. Dr. Reed was never told that morcellation would be performed during her surgery, or about the potential risks.
As a result of this surgical procedure with morcellation, a small cancer that could have been easily and completely removed through surgery has been spread and is now considered fatal.
Dr. Reed, who is now undergoing aggressive treatment for her metastasized uterine cancer, and her husband, Dr. Hooman Noorchashm, who was a surgeon at nearby Brigham and Women’s Hospital (also affiliated with Harvard), began a campaign to raise awareness of this issue and prevent other patients from being harmed. As a result, Brigham and Women’s Hospital has since changed its policies on use of morcellation. Since their story came out, other similar stories have surfaced, confirming that cancer has been spread by these devices, that it is not a rare event, and that it can have fatal results. Moreover, many of these patients had not been told about these potential risks before their surgeries, and in some cases weren’t even told that morcellation would be used. In May 2015, the Wall Street Journalreported that the FBI is investigating whether information about the risks of morcellation was not reported by hospitals, doctors, and device makers, as required by law.
What are uterine fibroids?
Uterine fibroids are non-cancerous (benign) growths on the uterus. They are very common among women, especially during and after the reproductive years. In many women, they do not cause any noticeable symptoms or problems. But in some women, uterine fibroids can cause pain, discomfort during sex, and heavy bleeding. To read more about fibroids and treatment options for them, read our in-depth article here.
What are the risks and benefits of using power morcellators?
Morcellation can allow surgeons to do shorter, less invasive surgeries. This can reduce the chances of excessive blood loss and infection, and can reduce the amount of time spent in the hospital and result in an easier recovery afterwards. However, in the case of fibroids, there is no way to rule out the chance of hidden cancer which could be spread by morcellation. The Food and Drug Administration (FDA) estimates that 1 in 350 women receiving surgery for uterine fibroids has a hidden cancer that could be spread by morcellation. This is why the FDA released a warning in April 2014 recommending against morcellation for uterine fibroids.
On July 10-11, 2014, the FDA held a public meeting to discuss the risks and benefits of these devices. Our testimony before the FDA panel on uterine morcellation, is here.
On November 24, 2014 the FDA announced that they were issuing an immediate change in the label for power morcellation devices, which will now include a black box warning as follows:
“Uterine tissue may contain unsuspected cancer. The use of laparoscopic power morcellators during fibroid surgery may spread cancer and decrease the long-term survival of patients. This information should be shared with patients when considering surgery with the use of these devices.”
These tragic events involving power morcellation devices raise questions about how medical devices are approved and monitored, and how a tragedy like this can be prevented in the future. If larger studies had been done before the FDA allowed these devices to be used, and if cases of cancer being spread by morcellation had been reported to the FDA by doctors and companies, the FDA could have warned doctors and patients much earlier and prevented women from being exposed to these risks.
What do patients need to know?
If you are considering surgical treatment for uterine fibroids, be sure to discuss morcellation with your surgeon and make your wishes clearly known. Depending on your particular situation, there are alternative surgical procedures, such as vaginal hysterectomy, which can be done without morcellation. For any surgical procedure, make sure you have a clear and thorough discussion with your doctor about exactly how the procedure will be done, what choices you have, and what the risks and benefits of different options are. If you feel that you are not getting enough information from your doctor, consider getting a second opinion. Be sure to ask your doctor how often they perform the procedure you will have, because patients usually have a better outcome from surgery if the doctor performs the exact same surgery frequently. If the physician does not have many years of frequent experience with the surgery, seek out a doctor who does. For more tips on how to make smart decisions about medical treatments, especially use of medical devices, read our article here.
When most people think of radiation, they think of manufactured devices such as the nuclear bomb or cancer treatments, which emit high doses of radiation. In reality, however, radiation takes many forms and is always around us. Some types are much more dangerous than others.1,2
Most researchers agree that there is no such thing as a dose of ionizing radiation that is so low that it will not have some effect on our body, such as damaging cells. Usually, the damage is small enough that one dose does not lead to any health problems. It is likely that the increased risk of cancer from low doses of radiation is so low that studies in the general population can’t detect it.3,4
It is important to note that each exposure to radiation builds up in our body and the risk of cancer increases with each radiation exposure. So even though a single source of exposure to radiation is unlikely to cause cancer by itself, the combined exposures add up throughout our lifetime and increase our risk of cancer over time.5 This is why it is important to limit unnecessary exposures to radiation. Radiation exposure during certain sensitive times of development, such as during childhood and puberty, also has more health risks than the same exposures in adults.6,7
Since radiation is always around us, we cannot avoid all radiation, but we can try to limit our exposures. This article will explain the various risks associated with different sources of radiation and how you can avoid getting too much exposure to radiation.
Background radiation refers to radiation that naturally occurs in our environment and does not come from any manufactured devices. Radiation is emitted from the earth, sun, our galaxy, and other galaxies. Even the human body naturally contains some radioactive elements.8People who receive few or no high-dose radiation medical tests usually get more exposure to radiation from the natural environment than from any manufactured device.9
This is because we are constantly exposed to a very low dose radiation for our whole lives, while devices such as x-ray tests expose you to radiation for a very short period of time. On the other hand, one CT scan can be equal to several years of background radiation exposures, so many people receive much higher doses of radiation from medical devices than they do from the natural environment.
The risk of developing cancer from a lifetime exposure of background radiation is about 1 in 100, or 1% of the population.10It is impossible to avoid all background radiation, but the best ways to limit unnecessary exposure to radiation from the environment is to prevent your exposure to radon and repeated unprotected sun exposure.
Radon
Radon is a color
less, odorless gas that comes from decaying rocks and soil. For the average person, radon accounts for over half their annual exposure to radiation. Radon comes up from the ground and gets trapped in houses and buildings.
Exposure to a small amount of radon inside is normal, but high levels can cause lung cancer. Radon is the second leading cause of lung cancer (smoking is the leading cause), and approximately 1 in every 15 houses have too much radon. The only way to know if you have a safe level of radon in your house is to get it tested.11
Cosmic and terrestrial radiation
Cosmic and terrestrial radiation is radiation that comes from the galaxy and from the earth. It makes up about 8% of our average yearly exposure to radiation.12 Cosmic radiation includes ultraviolet (UV) rays from the sun that cause tans and sunburns. UV rays can also damage the DNA in our skin cells and lead to skin cancer.13 Although we cannot avoid UV rays all the time, limiting exposure to direct sun light can reduce your risk of skin cancer. Tanning beds are also a common source of UV radiation and are just as dangerous as radiation from the sun. For more information on tanning beds, please read: Tanning Beds: Safe Alternative to Sun?
Being at higher altitudes, such as flying on a plane or living in a “mile high” location, will exposure you to higher levels of cosmic radiation than being at sea level. While there is technically no “safe” dose of ionizing radiation, the chances of getting cancer from frequent plane trips is very slim. Studies of airline crew members have not found a significant increase in risk of cancer after many years of working on airplane.14
In addition, living in Denver or other high altitude locations that receive higher doses of cosmic radiation has not been shown to increase the risk of cancer.15
How to Reduce Radiation Exposure from the Environment
Radon: Test the level of radon inside your house to make sure it is not too high. You can hire a professional to do this or you can purchase a “do-it-yourself” radon testing kit. It generally takes only a few minutes and is easy to do. If there is too high a level of radon in your house, people usually install an active soil depressurization (ASD) system, which is basically a ventilation system.2
UV Radiation: Some of the best ways to reduce your exposure to harmful UV rays are to:
Wear sunscreen (at least SPF 15) year-round in all areas of your body that are exposed to the sun. (However, it is good to get vitamin D from the sun for 15 minutes each day.)
Stay in the shade, especially when the sun is at it’s strongest (between 10am and 4pm)
Wear protective clothing, such as broad-brimmed hats and tightly-woven clothes that cover your hands and legs.
X-rays use ionizing radiation and are used for many types of diagnostic tests such as CT scans, mammograms, fluoroscopy, and simple x-rays. These tests allow your doctor to see potential problems inside your body and choose an appropriate treatment. They can help doctors make life-saving decisions, but some doctors are performing unnecessary scans or are using doses of radiation that are too high.16 Since x-rays use ionizing radiation, they can cause damage to our cells and DNA. X-ray tests can lead to cancer, but several common tests (such as mammograms and bone x-rays) use very low doses that have not been shown to cause a significant increased risk of cancer when administered properly.
Over the past few decades, the average level of radiation that Americans are exposed to has increased rapidly due to increased use of medical diagnostic tests such as x-rays (including dental x-rays and mammograms) and CT scans and cancer treatments. Diagnostic tests and treatments can help improve patients’ quality and length of life, but there are also risks. Usually, the benefit of receiving one of these tests outweighs the risk, but patients and doctors need to be wary of performing unnecessary tests, particularly if the test uses high doses of radiation.
Not all imaging tests use radiation that has been linked to cancer. Magnetic Resonance Imaging (MRIs) and ultrasounds do not use x-rays. Instead, they use non-ionizing radiation and have not been found to increase the risk of cancer or other health problems.17
MRIs and Ultrasounds are a safer alternative to diagnostics tests that use x-rays or other ionizing radiation.
Children, young adults, and fetuses of pregnant women should be particularly careful about getting any x-ray tests. Children, young adults, and fetuses are more sensitive to radiation, and their young age also allows a longer period of time for cancer to develop.18,19,20
Pregnant women should avoid any x-ray exposure, particularly when they are less than 20 weeks pregnant, since radiation exposure in the womb can lead to mental retardation, growth retardation, leukemia, and other cancers later in life.21 If it is necessary for a pregnant women to be x-rayed, the American College of Obstetricians and Gynecologists states a single x-ray test does not harm the fetus, but a protective lead apron should be used to cover the abdomen.22 However, high-dose, multiple-dose, or x-rays of the pelvic region should be avoided for pregnant women, whenever possible.
Many people get simple x-ray tests, such as an arm, leg, chest, or dental x-ray that look for broken bones or other problems. Simple x-ray tests use very low doses of radiation,23and studies have not found an increase risk of cancer among humans who have received a very low dose of radiation.24 Although the dose of radiation used to x-ray different parts of the body will vary, most simple x-rays use less radiation than other types of x-ray scans (such as a mammogram or CT scan).
While these doses of radiation could cause new cases of breast cancer, the appropriate use of mammograms has resulted in lives saved, and the benefits of getting regular mammograms are likely to be even greater than the risks when the frequency of mammograms is reduced to every other year.
Women who are carriers of the BRCA genetic mutation were previously recommended to begin yearly mammograms at age 25-30, since this mutation puts them at much higher risk of getting breast cancer. Newer studies have found that starting yearly mammograms before age 35 has no benefit to these women and may instead be harmful. They end up with higher exposure to radiation over their lifetime, which increases the chance of getting radiation-induced breast cancer that they may not have gotten otherwise.26
Fluoroscopy
Fluoroscopyis an x-ray test that allows doctors to see a continuous x-ray image of your body (like a movie, rather than just a picture as with other x-ray tests). Fluoroscopy uses an x-ray absorbing dye that is either drunk or injected into the body, which allows doctors to see a better outline of the organ. This procedure is used to view the digestive system (such as stomach, kidneys, or colon), arteries, or joints.27
Since this test sends x-ray beams over an extended period of time (usually 20-60 minutes),28 it exposes people to much higher doses of radiation than a simple x-ray test, although the doses vary widely depending on the test.
Fluoroscopy and CT scans both use high doses of radiation and pose the greatest and most avoidable risk of radiation-induced cancer. Limiting the number of CT and fluoroscopy tests you receive is one of the best ways you can avoid getting cancer from radiation. In addition to increasing cancer risk, this test can damage the skin and cause burns.29
Computed Tomographic (CT) scans
CT Scans are a relatively new type of diagnostic imaging technology that allows doctors to view 3-dimentional pictures of various organs in your body. CT scans use higher doses of radiation than most other types of diagnostic test and are likely to cause new cancers in some patients, compared to their risk if they had not received a CT scan.
Today, an American’s average lifetime dose of radiation from diagnostic procedures is six times higher than it was in the 1980s.30 This is largely due to the increased use of CT scans. Everyday, 19,500 CT scans are performed in the U.S. and this number continues to climb. Each CT scan is equivalent to 30 – 442 chest x-rays, depending on the dose used for the CT scan.31 One study projected that CT scans performed in the U.S. in 2007 alone will result in 29,000 new cancer cases and roughly 15,000 deaths that would not have occurred if they had not received a CT scan.32 These risks would increase with each additional CT scan a person receives. Low-dose CT scans, which expose patients to less radiation, are now being used to screen for lung cancer, with concerns about whether the benefits outweigh the risks. For more information on low-dose CTs, click here.
Unfortunately, there is no established guideline for how much radiation should be used for each procedure. Different scans require different levels of radiation in order to get a clear image, but some doctors are using more radiation than is necessary. One study found that different medical facilities had huge variations in the dose of radiation used for the same procedure. On average, the highest dose given for a CT scan was 13 times higher than the lowest does given for the same type of scan.33 The researchers found no pattern in why this dose variation occurred, and no scientific justification.
Children’s exposure to radiation from CT scans is particularly worrisome because children have many more years to develop cancer than adults receiving CT scans and are more sensitive to the effects of radiation. A June 2012 study found that children receiving higher doses of radiation — through multiple CT scans– were more likely to develop brain tumors and leukemia than children who had only one CT scan.34 However, brain tumors and leukemia are very rare conditions and the increased risk due to CT scans was relatively small: for every 10,000 CT scans performed on children under 10 years-old, there will be one additional diagnosis of leukemia and one additional diagnosis of a brain tumor. The researchers concluded that the benefits of children having necessary CT scans outweighed the risks of later developing cancer.
A study published in May 2013 looked at children from infancy to 19 years of age in Australia and compared those who had undergone CT scans to those who had never had any.35 Ten years after getting scanned, there were 24% more cases of cancer among the 680,000 children and teenagers who had CT scans than among the 10 million children and teenagers who did not undergo CT scans. Young people who had CT scans during the 12-month period before being diagnosed with cancer were not counted because the decision to scan them may have had to do with cancer symptoms. Children 4 and under had the highest increased risk in cancer, and risk for all increased with the number of scans. The researchers concluded that for every 1,800 people under 20 who had a CT scan, there was 1 additional case of cancer that would not have occurred without the radiation from the CT scan. The CT scans in this study took place between 1985 and 2005 when radiation doses where generally higher than they are today.
Parents should make sure that CT scans ordered for their children are medically necessary and ask their doctors if lower-radiation alternatives exist. While parents should not stop their children from receiving a necessary CT scan because of radiation concerns, they should think about keeping the number of scans below age 20 to a minimum.
The FDA and investigative journalists have also released warnings about occurrence of extreme accidental overdoses of radiation from CT scans.36,37
In January 2010, the FDA reported that over 250 patients at 4 facilities had received as much as 8 times the amount of radiation that they were supposed to receive.38 Accidental radiation overdoses can result in skin redness, hair loss, increased risk of various cancers and cataracts in the future, and death. While extreme overdoses of radiation are rare, these avoidable mistakes have lead many health professionals to call for more standardized and comprehensive methods of overseeing medical radiation.39
PET scans differ from other types of diagnostic imaging in that they allow doctors to see how an organ or system is functioning rather than just seeing the structure. This test works in a very different way than other tests and does not use x-rays-rather, it uses gamma rays, which usually have a higher level of energy than x-rays.
PET scans work by injecting (or swallowing) small amounts of radioactive material, which then spreads throughout the body. The PET scanner is then used to detect the radiation that is emitting from the radioactive material in your body. Procedures that use radioactive material to diagnose and treat patients is referred to as “nuclear medicine.”40
The dose of radiation from a PET scan is similar to CT, and therefore exposes people to a relatively high dose of radiation in comparison to other types of scans.
Using Radiation to Treat Cancer:
Radiation therapy
Radiation therapy uses high doses of radiation to treat various types of cancers. Beams of radiation are directed at the cancer to kill off cancerous cells. This can save lives and prevent recurrence of cancer, but healthy cells that are exposed to radiation may develop into a new cancer. Fortunately, new cancers caused by radiation therapy are not thought to be very common since radiation technology can precisely irradiate a small part of the body that contains cancer, minimizing the amount of healthy cells that are exposed to radiation.41
Another concern about radiation therapy and diagnostic tests are errors in using this technology. Although relatively uncommon, some patients will accidently receive doses that are too high. In addition to being at increased risk of developing cancer in the future, the incorrect doses can cause serious wounds to the skin, bone, and other organs, as well as death.42,43
Between 1950 and 2006, the frequency of diagnostic radiation increased 10-fold.44 As health professionals continue to find new uses for medical devices that use radiation, people will be exposed to radiation more often. For example, many radiologists have recently started promoting the use of CT scans to screen for colon cancer (known as a virtual colonoscopy), although the FDA has not approved CT scans for this purpose.45
Although many patients would prefer this non-invasive procedure over the traditional direct examinations, it would expose people to high doses of radiation that is roughly equal to 100 chest x-rays (or 3 years of background radiation.46 This means more people are likely to be diagnosed with cancers that are caused by radiation than they would not have gotten otherwise.
Backscatter and millimeter scanners have begun replacing metal detectors and are designed to scan a person to determine what weapons or explosives they may have beneath their clothing. Currently, there are about 250 backscatter and 264 millimeter wave scanners in the United States. The TSA hopes to have 1,800 scanners of either type installed by the end of 2014 – which would mean that nearly every airport in the country will have one.
Backscatter scanners look like two large blue boxes:
(Source: Transportation Security Administration)
People raise their arms and stand sideways between these two boxes when they are scanned.
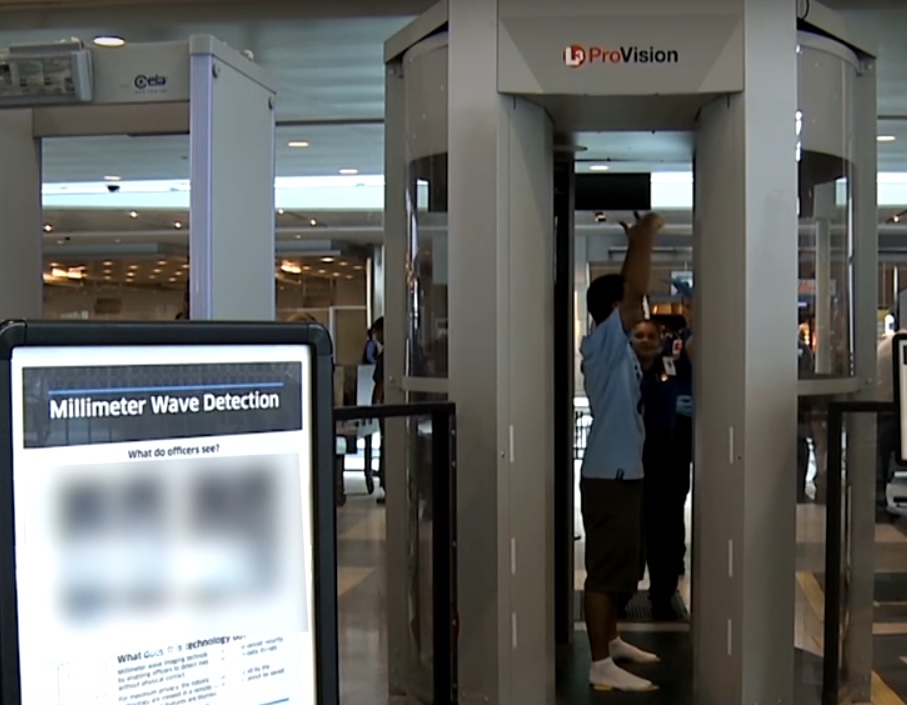
In contrast, millimeter wave scanners look like circular glass phone booths, and the person being scanned stands with their arms raised while part of the scanner rotates around them:
(Source: Transportation Security Administration, from http://www.tsa.gov/videos/travel-tips-advanced-imaging-technology)
If you are not sure which scanner is in use at your airport, ask a TSA official at the security checkpoint.
While metal detectors and millimeter scans both use non-ionizing radiation, which until recently was assumed to be safe (see our article Can Cell Phones Harm our Health?), backscatter scans use ionizing radiation, which is used in x-rays and known to potentially increase the risk of cancer. Backscatter scans work a little differently from x-rays. X-rays work by sending high-energy radiation to the body and recording the radiation that passes through the body. Dense parts of the body (like bones) block some of the radiation, resulting in lighter areas on the recorded image. Backscatter scanners also send radiation toward the body, but at much lower energy than an x-ray. Because it is not as strong as the radiation used in x-rays, the radiation does not pass through the body. Instead, the outer layers of the body “scatter” the radiation, which bounces off the body and back toward the machine. People receive most of the radiation that is absorbed by the body is deposited in the outer layers (like the skin and ribs), although a 2012 study showed that radiation from these scans may penetrate to other organs.47 Because the radiation is concentrated in the skin, there are concerns that this could cause skin cancer.
All data on backscatter scans are provided by TSA, a government agency that does not allow independent researchers to examine the machines they use.48 Researchers must therefore make educated guesses using data provided by the TSA, or they must make models of the scanners based on information that the agency releases.
The TSA states that backscatter scans use such low doses of radiation that estimating the potential effects of the scan is extremely difficult.49,50 A 2011 report using information from the TSA found that these backscatter scans expose people to the same amount of radiation that they receive from 3 to 9 minutes of normal daily life or from 1 to 3 minutes of flight.51 To put this into perspective, we would expect only 6 of the 100 million airline passengers each year to develop a cancer in their entire lives due to the backscatter scans.
Dr. David Brenner, a researcher at Columbia University, produced a different estimate based on the risk that the scanners are to the entire population, not just to an individual.52 Dr. Brenner multiplied the risk associated with one scan by the number of scans conducted each year to estimate the number of people who may develop cancer in one year because of the scanners. Because up to one billion scans may be performed each year, Brenner estimated that each year 100 people would develop cancer because of their exposure.
In April 2010, a group of scientists from the University of California, San Francisco wrote a letter of concern to Dr. John Holdren, the Assistant to President Obama for Science and Technology, about the backscatter scans. These researchers pointed out that because backscatter scans only penetrate outer layers of the body, it is possible that these layers receive a higher concentration of radiation than previously believed.
The scientists also expressed concern that sperm may mutate because the testicles are close to the surface of the skin and are exposed to radiation during these backscatter scans. In addition, they noted that the effects of radiation on the cornea (the outer surface of the eye) and the thymus (a part of the immune system located in the chest) have not been studied. While this letter only outlined concerns of the scientists and did not present new data, it called for further testing of backscatter scans. The scientists called for more rigorous and independent studies to ensure that the scans are safe for the entire population, as well as for all parts of the body.
In a joint reply with the TSA, the FDA stated that the radiation exposures from the backscatter scans were within established legal limits, even for frequent fliers.53 In reply to the scientists’ concerns that the radiation dose to the skin would be higher, the FDA wrote that their calculations showed that a person would have to pass through the scanner 1000 times in a year in order to begin to absorb the annual limit of what is considered safe.54
Not everyone agrees with the FDA, and some people have pointed out that TSA agents operating the scanners may improperly manage the devices or that mechanical errors may occur, either of which could cause the machines to emit more radiation than they are supposed to. From May 2010 to May 2011, there were 3,778 calls for mechanical problems on backscatter machines, but only 2% of those machines were evaluated for radiation safety.55
For a more in-depth look at airport security and radiation, read here.
Microwaves, Cell Phones, and Other Manufactured Devices
There is still much debate among scientists about whether non-ionizing (low-energy) radiation such as microwaves can increase your risk of cancer or other health problems. The concern is not about microwave ovens, but rather the long-term exposures to microwaves from other sources, such as communication towers and cell phones.56 Cell phones emit very low doses of microwave radiation, which was long assumed to be safe.
Although generally safer than ionizing radiation, the much longer-term exposure could make these products potentially dangerous. There are studies indicating that long-term exposures to low doses of non-ionizing radiation can damage DNA and may cause cancers and neurological and reproductive harm.57,58
Tobacco, fertilizer, welding rods, smoke detectors, and several other consumer products also contain some radiation, but radiation from these sources is generally very low (approximately 3% of our yearly radiation dose.[10]
APPROXIMATE DOSE AND CANCER RISK OF VARIOUS RADIATION SOURCES: How does it compare to natural background radiation? What is the lifetime risk of cancer death from one exposure to this radiation source?
Type of Radiation (dose in mSv)†
Equivalent Period of Natural Background Radiation‡
Estimated Lifetime Risk of dying from cancer that results from a single exposure§
Airport Security x-ray scanner23(~0.0001mSv)
less than one hour
Almost (less than 1 in 100,000,000)
7 hour airplane flight9(~0.03 mSv)
a few days
Almost 0 (1 in 1,000,000 – 100,000)
Chest x-ray6(~0.1 mSv)
~ one week
Almost 0 (1 in 1,000,000 – 100,000)
Mammogram (~0.4 mSv)
a few months (~2 months)
1 in 100,000 to 10,000
CT of chest27(~7 mSv)
a few years (~2.3 years)
1 in 10,000 to 1,000
Fluoroscopy: colon (barium enema)27(~8 mSv)
a few years (~2.7 years)
1 in 10,000 to 1,000
CT of heart (angiography)27(~16 mSv)
a few years (~5.3 years)
1 in 10,000 to 1,000
PET scan, whole body5(~14 mSv)
a few years (~4.6 years)
1 in 10,000 to 1,000
Fluoroscopy: kidneys, ureters and bladder5(~15mSv)
a few years (~5 years)
1 in 10,000 to 1,000
Whole-body CT scan5(~22.5 mSv)
several years (~7.5 years)
1 in 1,000
Nuclear Medicine: Cardiac stress-rest test (thallium)27(~40.7mSv)
Lifetime risk of cancer death NOT caused by radiation§§
1 in 5
†Dose is based on a normal effective dose for that type of scan. Actual doses used for a specified scan vary widely depending on the medical institution, the individual, and other factors.59
‡Natural background radiation is equal to about 3mSv per year.60
§ Risk of developing cancer is based on EPA cancer risk estimates: “…health physicists currently estimate that overall, if each person in a group of 10,000 people exposed to 1 rem [10mSv] of ionizing radiation, in small doses over a life time, we would expect 5 or 6 more people to die of cancer than would otherwise.”[33]
§§ “In this group of 10,000 people, we can expect about 2,000 to die of cancer from all non-radiation causes. The accumulated exposure to 1 rem [10 mSv] of radiation, would increase that number to about 2005 or 2006.”[33]
All articles are reviewed and approved by Dr. Diana Zuckerman and other senior staff.
The thought of cancer is so frightening that many patients depend on their physicians to make all the decisions about screening, prevention, and treatment. Or they may ask for whatever “new cure” they have heard about. That can result in too many tests or treatments that do more harm than good. Not every test, procedure, or medication is appropriate for every patient, and many are over-used. What is beneficial for one person isn’t worth the risks for another.
The best health decisions can be made when physicians take the time to talk with their patients and patients ask questions rather than just assuming the doctor always knows best.
The ABIM Foundation and Consumer Reports collaborated with specialty medical societies to create lists of “5 Things Physicians and Patients Should Question” as part of a national effort called Choosing Wisely (www.choosingwisely.org). These medical groups represent more than 500,000 physicians. The lists contain evidence-based recommendations made by experts. Here is the list of their recommendations on cancer.
Breast cancer screening
Breast cancer screening is done through mammograms, which are like x-rays. A breast cancer diagnosis involves giving the cancer a stage (0 through 4, with 4 being the most advanced) based on the size of the tumor, how advanced it is, and how likely it is to spread. Other imaging tests, like PET, CT, and bone scans are not recommended for screening early stage breast cancer (stages 0-3), patients newly diagnosed with Ductal Carcinoma In Situ (DCIS), or people without symptoms. This testing does not benefit patients, and false-positives (test results that indicate cancer when no cancer is present) can lead to unnecessary procedures and misdiagnosis. For anyone who has been treated for early-stage breast cancer and is symptom free, mammograms and regular clinical exams are the best ways to check that the cancer has not come back. Advanced imaging tests and tumor marker tests should only be used for patients with later-stage breast cancer.
Cancer therapy
The first round of cancer therapy works best at reducing or eliminating a tumor. Multiple treatments, including chemotherapy, will not always help get rid of cancer, especially more advanced cancers or tumors that return. After three different treatments, another round is unlikely to improve quality or length of life. It is better to stop therapy and not suffer through the side effects of treatment. (In fact, there is some evidence that patients live longer, with better quality of life, if they stop aggressive treatments earlier.)
Cervical cancer screening
Women over 65 should stop being screened for cervical cancer if they have not previously shown risk for disease. Women under 30 should not have HPV tests to screen for cervical cancer. Women with mild dysplasia or cervical intraepithelial neoplasia (CIN1) for less than two years should not be treated for cervical cancer, as CIN1 is usually caused by a short-term HPV infection and goes away within a year. See below for information about HPV testing. Pap smears should be used to screen for cervical cancer.
Colon cancer screening
For people who are at an average risk for developing colon cancer, tests such as stool tests and sigmoidoscopy can be used instead of colonoscopy to screen for colon cancer. Abnormal results from these tests require follow-up with a colonoscopy. The plasma test named methylated Septin 9 (SEPT9) is an alternative screening test but it is not recommended unless the more conventional tests and colonoscopy are not feasible.
HPV testing
HPV testing is not recommended for low risk infections, such as for HPV associated with genital warts. HPV testing should be used to identify high risk infections in patients with abnormal Pap smears or other clinical symptoms associated with high risk HPV infections.
Ovarian cancer screening
Women at average risk who do not have symptoms should not be screened for ovarian cancer. Screening using ultrasound or blood serum testing might detect early signs of cancer, but ovarian cancer is uncommon in women of average risk without symptoms. An abnormal result that isn’t cancer might require invasive follow-up, and those risks outweigh the benefit of early detection.
Ovarian cysts
Small, simple cysts are common in women and usually won’t affect their health. If one is found, the doctor will schedule an ultrasound to determine if the cyst is benign (not cancer). If the cyst is not cancerous, a follow up ultrasound and surgery is not recommended unless the cyst causes symptoms, like pelvic pain. If the cyst is suspected to be cancerous, a follow up ultrasound is not recommended because the cyst should just be surgically removed. A second ultrasound is only recommended for larger cysts that the doctor could not be sure about.
Palliative care for bone metastasis
Cancers that spread to bones are often very painful. Local radiation is sometimes used to treat patients with one or a few bone metastases, but some doctors question if the increased risk of cancer warrants radiation as treatment for pain. The American Society for Radiation Oncology recommends using one dose of radiation to relieve pain from any bone metastasis. While another dose might be needed in the future, starting with one dose makes sense, since patients with bone cancer have a short life expectancy.
Prostate cancer screening
Men who do not have symptoms generally should not be screened for prostate cancer using a prostate-specific antigen (PSA) test or digital rectal exam as it can lead to treatments that may do more harm than good. Gleason and prostate-specific antigen (PSA) tests are used to measure how aggressive prostate cancer is and how likely it is to spread. Imaging tests can then be performed to identify exactly where cancer has spread. These imaging tests, such as bone scans, PET, and CT, are not recommended for detecting disease in men who are newly diagnosed with low-grade prostate cancer. Imaging tests are expensive, can expose men to high levels of radiation, and are unlikely to provide more information about early prostate cancer. Only men with Gleason scores above 7 and PSA levels above 10 nanograms/mL should consider imaging tests.
Prostate specific antigen (PSA)
High PSA levels may be a sign of prostate cancer. However, having a low PSA level does not prevent prostate cancer nor does it mean there is no cancer. It was thought that antibiotics might lower PSA and protect men from prostate cancer. This has not been proven in clinical tests and is not recommended as an alternative preventive therapy.
Stage 1 non-small cell lung cancer (NSCLC)
Lung cancer is the most common type of cancer to spread to the brain. However, the chance of patients with Stage 1 lung cancer developing brain metastasis is very low. Because of the rate of false positives is much higher than the actual rate of brain metastasis, brain imaging by MRI or CT is not recommended for patients with stage 1 NSCLC unless they have neurologic symptoms.
Thyroid scans
Radioactive iodine is absorbed by the thyroid and can be used to give doctors a picture of what the thyroid looks like, how it is functioning, and if there are any nodules in the area.Imaging with radioactive iodine is not recommended for determining whether thyroid nodules are benign or cancerous unless the patient is hyperthyroid. Nodules should be biopsied if the thyroid functions normally.
Sonia Nagda, MD, MPH, Cancer Prevention and Treatment Fund
Recent media reports have raised fears that radiation from dental x-rays and mammograms increase the risk of thyroid cancer. Thyroid cancer rates have been increasing over the past 30 years, and this cancer affects women three times as often as men.[1] Is it true that dental x-rays and mammograms are to blame for the increase in thyroid cancer? Can a simple thyroid shield (an optional extension of the lead apron that blocks x-rays from reaching the neck) reduce the risk and put fears to rest?
Radiation in many forms-including x-rays, CT scans, sunlight, nuclear fallout (from atomic warfare or nuclear accidents such as Chernobyl) and even the radiation therapy that is used to treat cancer-can harm the DNA in the body and cause cancer. For more on this, see: Everything You Ever Wanted to Know About Radiation and Cancer but Were Afraid to Ask.
The thyroid gland is one of the organs most sensitive to the risk of radiation. Located in the neck directly over the trachea (the tube that brings air from the nose and mouth into the lungs)¸the thyroid gland makes two different hormones, known as T3 and T4, which are responsible for regulating energy and the body’s metabolism.
Background Radiation vs. X-Rays
We are all exposed to small amounts of radiation all the time. This is called “background” radiation. People who live in areas where radon gas is common or at high altitude have higher levels of background radiation.
For radiation to affect your thyroid and cause cancer, it has to reach your thyroid gland in sufficiently high doses-either from a big one-time dose (as from a nuclear disaster) or through many smaller doses. The closer the area being x-rayed is to the thyroid, the greater the amount of scattered rays that will reach it. Since the mouth is closer to the thyroid than the breasts, it makes sense that dental x-rays are more likely to affect the thyroid gland than mammograms, which are x-rays of the breast. On the other hand, dental x-rays expose patients to much less radiation than a mammogram: 0.005 millisieverts (mSv) for a dental x-ray, which is comparable to one day of natural background radiation, as compared with 0.4 mSv for a mammogram, which is comparable to 7 weeks of background radiation.[2]
Besides the dose, the age of the person being x-rayed or scanned is important. The thyroid gland is particularly sensitive to radiation during childhood and adolescence-when the gland is most active and a person’s body grows the most. As we age, the thyroid gland doesn’t work as hard, and the amount of radiation that it takes in becomes much smaller.
Dental X-Rays: a Risk for Thyroid Cancer or Not?
A study by Sara Schonfield and colleagues at the National Cancer Institute, published in 2011, compared the number of dental x-rays received by a group of thyroid cancer patients prior to their diagnosis with the number received by a group of similar individuals without thyroid cancer. Overall, those who had dental x-rays were twice as likely to develop thyroid cancer. More than 75% of the thyroid cancer patients were diagnosed before the age of 44. The more dental x-rays that a patient received, the more likely he or she was to develop thyroid cancer: the patients who received more than 10 x-rays had more than 5 times the risk of developing cancer than someone who had not had any dental x-rays.[1]
Mammograms: a Risk for Thyroid Cancer or Not?
The radiation that scatters from the breast to the thyroid gland is so negligible that the risk of developing thyroid cancer in a 40-year-old woman getting a mammogram is 6 in a billion.[3] This is similar to the amount of radiation your thyroid would get by standing outside for 30 minutes. Even if you got mammograms every year from the ages of 40 to 80, your risk of developing thyroid cancer would still only be 1 in 17.8 million, so there’s really no need to use a thyroid shield. In fact, using a thyroid shield during a mammogram makes the image blurry and more difficult for the radiologist to read. And, the thyroid shield can slip out of place and get in the way of the x-ray image, making a repeat exam (potentially exposing you to more radiation!) necessary.[4]
So, if mammograms don’t increase the risk of thyroid cancer, why are women three times as likely as men to be diagnosed with this cancer? Unfortunately, researchers have not yet found the answer to this question. Some believe that it could be related to better detection, and others think it could be a combination of diet, genetics, and the environment.[5]
Other Forms of Imaging
While CT scans of the head and neck are not as common as mammograms or dental x-rays, these can produce a lot of scattered radiation that can be absorbed by the thyroid. Studies have shown that wearing a thyroid shield during CT scans of the head and neck significantly limits radiation exposure to the thyroid gland.[6,7]
What You Need to Know to Keep You and Your Family Safe
Wear a thyroid guard during dental x-rays and CT scans.
You do not need to wear a thyroid guard during your mammogram. Continue regular mammography as recommended based on your breast cancer risk and age. Click here to learn about the latest mammography guidelines.
Try to keep x-rays of all kinds to a minimum, especially in children. Make sure that a scan (x-ray, CT, etc.) is being done only when needed, and that repeat exams are not done more frequently than absolutely necessary. Request that medical records and images be sent to all of the doctors treating you so that they don’t ask you to undergo scans that have already been done.
References:
Schonfeld SJ. Lee C. Berrington de Gonzalez A. “Medical Exposure to Radiation and Thyroid Cancer.” Clinical Oncology 2011; 23:244-250.
Chen AY, Jemal A, Ward EM. “Increasing Incidence of Differentiated Thyroid Cancer in the United States, 1988-2005.” Cancer 2009; 115(16): 3801-3807.
Williams L, Adams C. “Computed tomography of the head: An experimental study to investigate the effectiveness of lead shielding during three scanning protocols.” Radiography 2006; 12: 143-152.
Lee YH, Park E, Cho PK, et.al. “Comparative Analysis of Radiation Dose and Image Quality Between Thyroid Shielding and Unshielding During CT Examination of the Neck.” AJR 2011; 196:611-615.
Brandel France de Bravo, MPH, Kousha Mohseni, MS, Cancer Prevention and Treatment Fund
When we hear “sleeping pills,” most of us think of prescription drugs such as Ambien (generic name zolpidem), Restoril (temazepam), and Lunesta (eszopiclone). While prescription sleep medications are big business — more than $41 billion/year in the U.S. many people with trouble sleeping turn to over-the-counter antihistamines such as Tylenol PM and Benadryl.[1] However, the use of these drugs may take a nosedive in light of the findings of a study published in the prestigious British Medical Journal. Led by researchers at the Scripps Clinic Viterbi Family Sleep Center in California, the study shows that people who take these drugs are significantly more likely to be diagnosed with cancer or to die within the next two and a half years than people who don’t take them. Author Dr. Daniel Kripke estimates that these popular sleep medications could cause 320,000 to 507,000 deaths in just one year.
The researchers looked at 10,529 primary care patients who were prescribed sleeping pills between 2002 and 2007 and compared the health of each of them to at least two very similar patients without such prescriptions who were the same sex, ethnicity, marital status, smoking status, and had similar health conditions, alcohol use and BMI (which measures if a person is overweight). The patients were followed for 2.5 years on average, and were from a Pennsylvania clinic that serves a mainly low-income population.
Sleeping Pills, Death, and Cancer
Patients who were prescribed sleeping pills were at least three to five times more likely to have died during the study than were the patients not prescribed sleeping pills. Even the patients who were prescribed fewer than 18 pills per year were at higher risk of dying: 3.6 times higher. Patients who were prescribed more than 132 pills a year were more than five times as likely to die.
The researchers were careful to exclude from the study patients who were diagnosed with cancer before the study or very early in the study. Heavy users of sleeping pills (over 132 pills prescribed per year) had a 35% greater risk than those with fewer pills prescribed. Among those with prescriptions for sleeping pills, the increased risk of their developing lymphoma, lung cancer, colon and prostate cancer was greater than the risk from being a current smoker.
Before this study, there were at least 18 other studies showing an increased risk of death for people taking sleeping pills, and several also showed an increased risk of cancer. However, this study is especially well-designed and the only one that includes the newer, short-acting class of popular sleeping pills known as nonbenzodiazepines. These were generally believed to be safer than previous generations of sleeping pills because they wear off more quickly. In fact, before this study it was believed that the worst side effect was weight gain due to night time raids on the refrigerator while sleep walking.
Among study participants, the most commonly prescribed sleeping pill was zolpidem (sold as Ambien, Edluar, or Zolpimist), followed by temazepam (a benzodiazepine sold as Restoril). However, prescriptions for the use of any sleep aid was associated with a significant increase in the risk of death, including eszopiclone (”Lunesta”), zaleplon (”Sonata”), barbiturates, as well as antihistamines such as diphenhydramine (the active ingredient in Benadryl), which is also used in many over-the-counter sleep aids. The average age of patients was 54, but the study found harm associated with sleeping pill use in every age group.[2]
All the sleeping pills showed a similar increased risk of death except Lunesta, which showed a more than 500% increased risk compared to any of the other sleeping pills. However, Lunesta was a relatively new drug at the time of the study, and relatively few people took it. For that reason, it is not possible to say whether the risk of Lunesta is really that high. Also important to note: This study did not evaluate cancer among patients taking Belsomra, a newer sleeping aid with numerous side effects.[3]
One shortcoming of the study is that getting a prescription for a sleeping pill is not the same as taking sleeping pills. It is possible that some of the people with prescriptions, especially for small numbers of pills, never took any of them. It is also possible that people who did not have prescriptions for sleeping pills took Benadryl or other over-the-counter antihistamines to help them fall asleep, instead of the prescription version of the same pills. However, those shortcomings would tend to underestimate the risk of sleeping pills, rather than overestimate the risks.
In addition to the major study cited above, there is other evidence linking sleeping pills to cancer. For example, a study of Taiwanese patients published in 2012 found that Ambien promoted viral infections, which reflects a weakening of a person’s ability to fight off infections and diseases.[4] That could explain the increased risk of cancer.
Also, a study published in the Korean Journal of Family Medicine in 2018 found that sleeping pills were strongly associated with esophageal, kidney, prostate, liver, stomach and pancreatic cancers. Of all the sleeping pills in the study, Ambien most strongly predicted a diagnosis of cancer.[5]
But Why?
What could possibly explain these increased risks? Are people who are prescribed sleeping pills more anxious or stressed out? There is evidence that they are more likely to have car accidents or to fall down, probably because of the residual effects of the drugs during the day. Other studies show an increase in infections among people taking sleeping pills, and that can also increase the risk of cancer and death from other causes. These other studies all suggest that sleeping pills really do increase the risk of dying and there are no logical explanations to explain away the substantial increased risks found in this study, especially the increased risk of cancer.
While the researchers can’t say for sure that the sleeping pills caused death or cancer, many people who used to take these medications should think about these new research findings and consider other, safer ways to fall asleep. The sleep specialists who conducted the research suggest that since these sleeping pills have limited benefits, old-fashioned sleep aids like warm milk, as well as cognitive-behavioral approaches that can be taught and used for the rest of your life, would be excellent alternatives. If you decide to toss your sleeping pills, be sure to see our article Drugs in the Drinking Water for tips on safe medicine disposal.
All articles are reviewed and approved by Dr. Diana Zuckerman and other senior staff.
Kao, C.-H., Sun, L.-M., Liang, J.-A., Chang, S.-N., Sung, F.-C., & Muo, C.-H. (2012). Relationship of Zolpidem and Cancer Risk: A Taiwanese Population-Based Cohort Study. Mayo Clinic Proceedings, 87(5), 430–436. http://doi.org/10.1016/j.mayocp.2012.02.012
Kim, D.-H., Kim, H.-B., Kim, Y.-H., & Kim, J.-Y. (2018). Use of Hypnotics and Risk of Cancer: A Meta-Analysis of Observational Studies. Korean Journal of Family Medicine, 39(4), 211–218. http://doi.org/10.4082/kjfm.17.0025
Caroline Novas, Cancer Prevention and Treatment Fund
Anemia drugs are widely used by patients undergoing chemotherapy and patients with chronic kidney disease, but there is growing evidence that the misuse of these drugs is harming many patients. The FDA issued a “safety communication” on June 24, 2011 recommending lower doses of anemia drugs for patients with chronic kidney disease. This warning was based on studies showing increased risk of stroke, blood clots, other cardiac problems, and death for patients with chronic kidney disease.1
Procrit, Aransep, and Epogen are Erythopoiesis-Stimulating Agents (ESAs), which refers to synthetic versions of a protein that increases the production of red blood cells. By increasing red blood cells, these drugs reduce the need for blood transfusions.
The latest FDA “communication” again raises concerns about the safety of these drugs for any use, including patients with anemia due to chemotherapy. Studies show that cancer patients who receive ESAs have worse outcomes than patients who do not, because of higher mortality rates as well as faster cancer progression. In addition, evidence presented at a 2008 FDA meeting showed that only one in three cancer patients benefit from taking ESAs.2 The FDA requires this information on the labels for these drugs, but they continue to be widely used.
Procrit, Aranesp, and Epogen are multibillion dollar sellers manufactured by Amgen Inc.3 These drugs were approved by the FDA to treat anemia caused by chronic kidney condition in 1989 and chemotherapy in 1993.4
What is the connection between chemotherapy and anemia? Chemotherapy eliminates cancer cells but also attack healthy red blood cells. When a person’s red blood cell count falls very low, anemia is the result.3 In fact, seven out of ten chemotherapy patients develop anemia.5
In 2007, the FDA required warning labels for ESAs to treat patients with cancer and chronic kidney disease. The labels emphasize the risk of tumor growth and shortened survival when prescribed at a high dosage. Additionally, the warning label states that “symptoms of anemia, fatigue, and quality of life have not been shown to improve in patients with cancer who are treated by ESAs.”6
In 2010, the FDA finally responded to the studies showing increased tumor growth and shortened survival time. Although the FDA did not take the drugs off the market, they did issue a drug safety recommendation to recommend a risk management strategy program to improve safety for patients who have anemia due to chronic kidney disease and chemotherapy. Oncologists treating cancer patients must now undergo training before prescribing the drug. It also required that patients sign a written acknowledgment stating that the doctor has explained the risk of taking the drug.2
Given the FDA statement that ESA drugs do “not improve fatigue, patient well-being, or quality of life” and that the drugs only benefit one in three cancer patients,2 why does the agency allow cancer patients to continue taking the drug? They do so because there is no doubt that ESAs can reduce the need for blood transfusions. In addition, some patients respond very well to the drugs, and do not experience the side effects of increased tumor growth.7 As a result, for many patients the benefits of reduced blood transfusions outweigh the risks of tumor growth and increased mortality rates. The problem is that it often isn’t possible to determine which patients are likely to benefit and which are more at risk. In other words, for many patients, ESAs are a gamble.
If you are taking any of these drugs because of either chronic kidney disease or chemotherapy, talk to your doctor to see if the benefits of staying on the drug are likely to outweigh the risks. Make sure your doctor is aware of the FDA’s latest concerns and the research evidence of serious risks. You might consider asking your doctor about going off the drug to see if you are better off without it.
4Centers for Disease Control and Prevention. National Chronic Kidney Disease Fact Sheet: General Information and National Estimates on Chronic Kidney Disease in the United States, 2010. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2010.
Margaret Aker, Cancer Prevention and Treatment Fund
Has your child been to the orthodontist this year? Was he or she exposed to dangerous levels of radiation?
According to research reported in the New York Times,[1] more and more dentists and orthodontists are using an imaging device that delivers significantly higher doses of radiation than regular X-rays. While people usually don’t have any immediate problems from such radiation, exposure can be harmful over the long-term and has been linked to an increased risk of developing cancer.[2]
Promoters of the cone-beam CT scanner claim that this technology is a safe way to obtain highly detailed images of a patient’s mouth and skull that can be used to help treat complicated dental problems more accurately. Health experts, however, are concerned about the cumulative effects of radiation from these scans, and think they shouldn’t be used routinely.
For patients with more serious dental issues, such as cases involving implants or impacted teeth, the scanner’s comprehensive images may justify the radiation exposure. But in most cases, traditional X-rays, which expose patients to far lower levels of radiation, provide perfectly adequate images. It is worrisome, therefore, that some orthodontists, apparently misinformed about the risks of these scans, are using the cone-beam technology to scan all patients-many of whom are children.
The use of the cone-beam CT scanner is even more controversial for children, because they are more susceptible to the effects of radiation than fully developed adults. These scans put children at greatest risk for several reasons: they are smaller, their bodies are still developing, and the earlier they begin getting scanned, the more exposure they are likely to have over their lifetime. The main concern is cumulative exposure, not just a single strong dose of radiation.
In addition to the cone-beam scanner, there is also concern about the safety of X-rays taken during annual visits to the dentist. Despite a national campaign to reduce radiation levels to those absolutely necessary for proper imaging, many dental offices are still using outdated X-ray machines that emit more radiation than the newer machines. As evidenced by the cone-beam CT scanner, newer does not, of course, always mean less radiation.
Misuse or overuse of the cone-beam CT scanner also points to a much larger issue that has nothing to do with radiation: the extensive financial relationships that exist between doctors and the companies that make medical products. When manufacturers and doctors get too cozy, conflicts of interest arise, and patient care suffers. The cone beam scanners have become popular, in large part, because the machine’s primary manufacturer, Imaging Sciences International, has paid dentists and orthodontists to promote it. Although these health professionals may endorse the use of this scanner because they truly believe in its benefits, their enthusiasm may be influenced by these payments and the biased information they receive from the companies that make them. After a health professional has received a check, a dinner, or been to a conference at a fancy hotel with all expenses paid, dozens of research studies show that his or her opinion on a given product will probably be more positive than it otherwise would have been.
It is true that each scan only very minimally increases the risk of cancer. Unfortunately, the risk of these scans adds up quickly if every other trip to the orthodontist or dentist requires one. Dentists, orthodontists, patients, and parents need to ask: is this really needed? Especially when the patient is a child and when safer options are available, is the additional exposure to radiation really worth it?
This article, written by Adriane Fugh-Berman of Georgetown University Medical Center, which appears in the September 2010 issue of PLoS Medicine, reveals the ethically questionable ways in which Wyeth Pharmaceuticals promoted Prempro, a menopausal hormone replacement medication.
Wyeth paid highly respected physicians to allow their names to be listed as authors of research studies, reviews, commentaries, and letters to the editor, although they had not actually conducted or analyzed the research nor written the articles. These articles were published in medical journals and widely quoted, persuading doctors that hormone therapy was necessary and beneficial to reduce the detrimental effects of menopause and aging on women. Research subsequently proved that most of the “benefits” were unfounded, and that the truth was sometimes exactly the opposite of the claims: for example, hormone therapy had a negative rather than positive impact on memory.
Stephanie Portes-Antoine and Brandel France de Bravo, MPH, Cancer Prevention and Treatment Fund
Because of the risks of breast cancer, stroke, and other serious health problems, experts warn that women should only use hormone replacement therapy if the symptoms of menopause are causing major problems in their quality of life. In those situations, they should use the lowest possible dosage for the shortest period of time.[1] As a result of decreased use of hormone therapy, the breast cancer rate has declined in the United States in recent years. Nevertheless, the combined form of hormone therapy—consisting of estrogen and progestin—is still used by about 15% of postmenopausal women, with more than 25 million prescriptions written every year.[2]
As of June 2009, there is yet another reason to avoid taking hormone therapy. New research shows that hormone therapy can increase a woman’s chance of dying from lung cancer. Lung cancer is the leading cause of cancer deaths in women.
A large government study of post-menopausal women, called the Women’s Health Initiative (WHI), has been the major source of scientific information about the risks of hormone therapy since 2002. A new analysis published in June 2009 found that women who took hormone replacement therapy for five or more years were more likely to die of non-small cell lung cancer than women in the study who did not take hormone therapy.[3] Non-small cell lung cancer accounts for 85% of all lung cancer cases.
There were 16,000 women participating in the WHI study, ages 50 to 79, who either took Prempro, a drug combining estrogen and progestin, or took a placebo. Smoking rates were similar in both groups: half had never smoked, 40% were past smokers, and 10% were current smokers.
The risk of developing lung cancer was similar in both groups, but the women taking the hormones were about 60% more likely to die of lung cancer than the women taking a placebo. Not surprisingly, the risk was highest for current smokers, followed by past smokers, and lowest for never smokers. Among the women who smoked (former or current smokers), 3.4% of those taking hormone therapy died of lung cancer compared to 2.3% for women taking the placebo.
Among women who never smoked, 0.2% of hormone users died from lung cancer, compared with 0.1% of those who got the placebo. While the risk of dying from lung cancer was very small for women who never smoked, almost twice as many women died in the hormone group than in the placebo group. Because of the small number of non-smokers who died from lung cancer in this study, the increase is not statistically significant, which means it could have happened by chance. Research with larger samples is needed to tell us whether even non-smokers are at greater risk of lung cancer if they take hormone therapy.
These findings are consistent with previous research suggesting a link between hormone therapy and non-small cell lung cancer.[4,5] In the Journal of Clinical Oncology in 2006, Dr. Apar Kishor Ganti and his colleagues at the University of Nebraska reported that women with lung cancer who used hormone replacement therapy did not live as long as women who did not use hormones, even though the women receiving hormone therapy were younger.[6] Hormone therapy’s effect on survival was especially pronounced for women with a history of smoking.
According to Dr. Karen Reckamp, assistant professor of medicine at City of Hope Cancer Center in Duarte, California, “We see more and more non-smoking women getting lung cancer in general and often younger women. We know that there are estrogen receptors in the lung and in lung cancers and so there’s definitely an interaction between the development of lung cancer and hormones.”[7] The results from the Women’s Health Initiative study indicate that for most women, the risks of hormone therapy are much higher than the benefits, and we now know this is especially true for women who smoke or used to smoke.
Chlebowski RT et al. Non-small cell lung cancer and estrogen plus progestin use in postmenopausal women in the Women’s Health Initiative randomized clinical trial. Journal of Clinical Oncology, 2009 ASCO Annual Meeting Proceedings (Post-Meeting Edition). Vol 27, No 15S (May 20 Supplement), 2009: CRA1500.
Negaard HFS, Eilertsen AL, Anders DA, Iversen PO. Decreased Lung Cancer Survival with Hormone Replacement Therapy: Caused by a Decreased Tissue Factor Pathway Inhibitor Level? Journal of Clinical Oncology. June 10, 2006; 24(7): 2683-2684.
Siegfried JM. Hormone Replacement Therapy and Decreased Lung Cancer Survival. Journal of Clinical Oncology. January 1, 2006; 24(1): 9-10.
Ganti AK, Sahmoun AE, Panwalkar AW, Tendulkar KK, Potti P. Hormone Replacement Therapy is Associated with Decreased Survival in Women in Lung Cancer. Journal of Clinical Oncology. January 1, 2006; 24(1):59-63.
Karen Reckamp, M.D, assistant professor of medicine, thoracic oncology division, City of Hope Cancer Center, Duarte, Calif. May 30, 2009, American Society of Clinical
Julie Bromberg, Cancer Prevention and Treatment Fund
Heart disease is the leading cause of death among adults in the U.S., so some doctors have recently started using Computed Tomography (CT scanning, or “CAT scan”) to detect blockages in the heart’s arteries that can cause heart attacks. Unfortunately, a CT scan uses relatively large doses of radiation-an average heart CT scan exposes a patient to 23 times as much radiation as a chest x-ray.[1,2]
Researchers warn that if this test is widely used, we could see many new cases of cancer from increased exposure to radiation.
Doctors usually decide if a patient has a high or low risk for heart disease by assessing the person’s “risk factors” for heart disease. A “risk factor” is a behavior or characteristic that makes it more likely that a patient will get a certain disease.
People who have a higher risk of heart disease have some of the following risk factors:
unhealthy diet,
smoke tobacco,
high cholesterol,
high blood pressure,
older age, and several other risk factors
Patients with these high risk factors are more likely to have blocked or narrowed arteries, which can prevent blood flow and are a major cause of heart attacks and strokes. Doctors often recommend medication to people who have a high risk of heart disease, in addition to lifestyle changes such as healthier diet, exercise, and quitting smoking, which can help everyone prevent heart disease.
Even with information about cholesterol and blood pressure, however, doctors cannot always predict who will have blocked arteries. Some people who appear to be at low risk (for instance, non-smokers with low cholesterol) may have a build up in their arteries and could suffer from a heart attack. The heart CT scan has the advantage of detecting blockages in patients who seem to have a low risk of heart disease. One preliminary analysis found that the heart CT scan could prevent 9,000 more deaths than doctors’ traditional way of assessing risk factors while other studies have found that CT scanning does not actually improve health outcomes.[3,4,5]
The American Heart Association, American College of Cardiology, and the United States Preventive Services Task Force do not recommend the use of heart CT scans for patients with a low or high risk of heart disease because CT scans could be more harmful than beneficial due to the relatively high dose of radiation.[6,7]
In contrast, the Screening for Heart Attack Prevention and Education (SHAPE) guidelines recommend that heart CT scans be used to detect blockages in arteries of older men and women who do not have symptoms of heart disease. SHAPE’s guidelines lack scientific support, however, and although well-respected doctors helped write the guidelines, SHAPE is funded by several drug companies that could profit from increased use of heart CT scanning.
If doctors follow SHAPE’s recommendation, tens of millions of adults would be exposed to relatively high levels of radiation through this procedure. Doctors still have not established a standard dose of radiation to be used for heart CT scans and doses for this test vary from one hospital to another, with some patients getting 10 times the amount of radiation as patients in another hospital. A 2008 study estimated that one heart CT scan for the 50 million Americans who would be affected by SHAPE’s guidelines could cause 2,700-37,000 new cancer cases, depending on the dose of radiation. (Assuming the average radiation dose, these scans could result in 5,600 new cancer cases).[9] The number of new cancer cases could be even higher if individuals were screened more than once in their lifetime.
Radiation from CT scans is of concern to the FDA even when the CT scans are necessary. On October 9, 2009, the FDA announced that it was notifying healthcare professionals that 206 patients who were being tested for stroke received CT radiation doses that were approximately eight times the expected level at one particular medical facility. While this event involved a single kind of diagnostic test at one facility, the FDA warned that “it may reflect more widespread problems with CT quality assurance programs.”
Bottom Line
Each year, over 600,000 Americans die from heart disease even though heart disease can be prevented. Although heart CT scanning may be a useful tool in detecting blockages in heart arteries, there is not enough evidence to show that this test is worth the risks, especially compared to traditional risk factor assessment.[10,11]
For this reason, the Cancer Prevention and Treatment Fund of the National Research Center for Women & Families agrees with the U.S. Preventative Services Task Force that heart CT scans are not recommended for screening for heart disease. And, we agree with the FDA that doctors need to ensure that the risks of radiation from CT scans do not outweigh the benefits of testing.
There are several safer steps you can take to prevent heart disease:
Eat healthy foods
Exercise
Stop smoking
Reduce your stress as much as possible
If you have high cholesterol and/or blood pressure, talk to your doctor about how to manage it.
Kim KP, Einstein AJ, and de Gonzalez AB. Coronary Artery Calcification Screening: Estimated Radiation Dose and Cancer Risk. Archives of Internal Medicine, July 13, 2009; 169(13): 1188-1194.
Diamond GA and Kaul S. The Things to Come of SHAPE: Cost and Effectiveness of Cardiovascular Prevention. The American Journal of Cardiology, April 2007; 99(7)
Waugh N, Black C, Walker S, McIntyre L, Cummins E, and Hillis G. The Effectiveness and Cost-Effectiveness of Computed Tomography Screening for Coronary Artery Disease: Systematic Review. Health Technology Assessment, 2006; 10(39): iii-iv, ix-x, 1-41.
Gibbons RJ and Gerber TC. Calcium Scoring with Computed Tomography: What is the Radiation Risk? Archives of Internal Medicine, July 13, 2009; 169(13): 1185-1187.
Bluemke DA, Achenbach S, Budoff M, Gerber TC, Gersh B, Hillis LD, Hundley WG, Manning WJ, Printz BF, Stuber M, and Woodard PK. Noninvasive Coronary Artery Imaging Magnetic Resonance Angiography and Multidetector Computed Tomography Angiography: A Scientific Statement From the American Heart Association Committee on Cardiovascular Imaging and Intervention of the Council on Cardiovascular Radiology and Intervention, and the Councils on Clinical Cardiology and Cardiovascular Disease in the Young. Circulation, July 2008; 118: 586 – 606.
Barclay L. SHAPE Task Force Recommends Noninvasive Cardiac Screening for Asymptomatic Adults. Medscape Medical News, July 13, 2006.
Kim KP, Einstein AJ, and de Gonzalez AB. Coronary Artery Calcification Screening: Estimated Radiation Dose and Cancer Risk. Archives of Internal Medicine, July 13, 2009; 169(13): 1188-1194.
Kung HC, Hoyert DL, Xu J, and Murphy SL. Deaths: Final Data for 2005. National Vital Statistics Reports. 2008;56(10).
Waugh N, Black C, Walker S, McIntyre L, Cummins E, and Hillis G. The Effectiveness and Cost-Effectiveness of Computed Tomography Screening for Coronary Artery Disease: Systematic Review. Health Technology Assessment, 2006; 10(39): iii-iv, ix-x, 1-41.
Gibbons RJ and Gerber TC. Calcium Scoring with Computed Tomography: What is the Radiation Risk? Archives of Internal Medicine, July 13, 2009; 169(13): 1185-1187.