Laura Gottschalk, PhD, John-Anthony Fraga, Jared Hirschfield, Diana Zuckerman, PhD, National Center for Health Research
Electronic cigarettes, or e-cigarettes, are being marketed as the “safe” new alternative to conventional cigarettes. By February 2020, reports of 68 deaths and more than 2,800 vaping-related hospitalizations due to lung illnesses have made it clear that vaping can be even more dangerous than smoking.1,2
The CDC has reported that Vitamin E acetate is a potential cause for the outbreak, but it might not be the only one.2 Many of the patients report vaping marijuana products or marijuana and nicotine products, but others only vaped nicotine products. Until these reports of hospitalized teens and adults are scrutinized in greater depth, we won’t know what types of vaping are most dangerous and under what circumstances.
E-cigarettes come in a variety of forms and include vape mods, Juuls, and vape pens. There are brand name products (Juul is the most widely used) and “home-made” versions. Some contain high levels of nicotine, while others contain marijuana or just contain flavoring. The focus of this article is on e-cigarettes because most of the research that exists has been done on them, but much of the information below is relevant to these other products as well.
The big questions are: Are they safe? Will they reverse the decline in smoking—giving new life to an old habit—or can they help people quit smoking? Here is what you need to know.
What are E-cigarettes?
E-cigarettes are battery-operated devices that were initially shaped like cigarettes, but now include vape mods, Juuls, and vape pens. Some look like flash drives or highlighter pens, making it easy for teens to hide them in plain sight. The brand-name products contain nicotine, an addictive drug that is naturally found in tobacco and that stimulates, causes stress during withdrawal, and then feels relaxing as continued exposure follows withdrawal. It is the nicotine in cigarettes that makes smoking so addictive, and the same is true for most vaping and juuling. These electronic products allow nicotine to be inhaled, and they work by heating a liquid cartridge containing nicotine, flavors, and other chemicals into a vapor. Because e-cigarettes heat a liquid instead of tobacco, what is released is considered smokeless.3
Is Vaping Safer than Smoking Traditional Cigarettes?
The key difference between traditional cigarettes and e-cigarettes and related products is that the latter don’t contain tobacco. But, it isn’t just the tobacco in cigarettes that causes cancer and other serious diseases. Traditional cigarettes contain a laundry list of chemicals that are proven harmful, and e-cigarettes have some of these same chemicals.
While smoking can cause lung cancer, breast cancer, emphysema, heart disease, and other serious diseases, those diseases usually develop after decades of smoking. In contrast, in 2019 it became clear that vaping could cause seizures and serious lung damage after just a year, possibly less, based on CDC reports of patients hospitalized for lung damage caused by vaping.2,3 While there have been warnings about the possible risk of e-cigarettes for a decade, it was not expected that they could cause such severe damage in such a short period of time.
The COVID-19 pandemic has raised even more concerns about the safety of vaping. Youths aged 13-24 years old who have used e-cigarettes are more likely to be diagnosed with COVID-19, be tested for the virus, and to experience Covid-19 symptoms.4
Since 2009, FDA has pointed out that e-cigarettes contain “detectable levels of known carcinogens and toxic chemicals to which users could be exposed.” For example, in e-cigarette cartridges marketed as “tobacco-free,” the FDA detected a toxic compound found in antifreeze, tobacco-specific compounds that have been shown to cause cancer in humans, and other toxic tobacco-specific impurities.5 Another study looked at 42 of these liquid cartridges and determined that they contained formaldehyde, a chemical known to cause cancer in humans.6 Formaldehyde was found in several of the cartridges at levels much higher than the maximum EPA recommends for humans. In 2017, a study published in the Public Library of Science Journal showed that significant levels of benzene, a well-known carcinogen, were found in the vapor produced by several popular brands of e-cigarettes.7
The body’s reaction to many of the chemicals in traditional cigarette smoke causes long-lasting inflammation, which in turn leads to chronic diseases like bronchitis, emphysema, and heart disease.8 Since e-cigarettes also contain many of the same toxic chemicals, there is no reason to believe that they will significantly reduce the risks for these diseases.
In fact, a preliminary study presented at the 2018 annual meeting of the American Chemical Society found that vaping could damage DNA.9 The study examined the saliva of 5 adults before and after a 15-minute vaping session. The saliva had an increase in potentially dangerous chemicals, such as formaldehyde and acrolein. Acrolein has been proven to be associated with DNA damage, for example, and DNA damage can eventually cause cancer.10
A study of mice funded by the National Institutes of Health found that e-cigarette smoke could cause mutations in DNA that could increase the risk of cancer. These specific mutations have been shown to potentially contribute to the development of lung and bladder cancer in mice exposed to electronic cigarette smoke. The researchers claim that these chemicals could also induce mutations leading to cancer in humans. It has not been reported how many of those harmed had used juul devices. While many of those harmed had vaped marijuana, many also used nicotine e-cigarettes,11 so the risks of “juuling” need to be carefully and immediately studied.
Because they are smokeless, many incorrectly assume that e-cigarettes are safer for non-smokers and the environment than traditional cigarettes. However, a study published in the International Journal of Hygiene and Environmental Health found that the use of e-cigarettes results in increased concentrations of volatile organic compounds (VOCs) and airborne particles, both of which are potentially harmful when inhaled.12 Although e-cigarette vapor may not result in the obvious smell and visible smoke of traditional cigarettes, it still has a negative impact on air quality, especially when vaping indoors.
There are no long-term studies to back up claims that the vapor from e-cigarettes is less harmful than conventional smoke. Cancer takes years to develop, and e-cigarettes were only very recently introduced to the United States. It is almost impossible to determine if a product increases a person’s risk of cancer or not until the product has been around for at least 15-20 years. Despite positive reviews from e-cigarette users who enjoy being able to smoke them where regular cigarettes are prohibited, very little is known about their safety and long-term health effects.
There is also danger from e-cigarettes exploding in the user’s mouth or face. Last year, the British Medical Journal used data from several agencies to estimate that there were roughly 2,035 e-cigarette explosions and burn injuries in the U.S. just in a three-year period from 2015 to 2017. One of the authors of the study stated that the number was likely higher as such incidents were not well tracked. The report also said that e-cigarettes, commonly powered by a lithium-ion battery, could overheat to the point of catching fire or exploding, a phenomenon known as “thermal runway.”13
Can Vaping Help to Cut Down or Quit Smoking Regular Cigarettes?
Recent research provides conflicting evidence on whether vaping helps people quit smoking, with differences in results apparently due to changes in how the studies were designed and conducted. A 2025 study followed more than 6,000 adult smokers from 2017 to 2021 and found that those who vaped every day were not significantly more likely to quit smoking than those who didn’t vape at all.14 The results were based on the Population Assessment of Tobacco and Health (PATH), a large, ongoing government-funded study tracking tobacco use and health outcomes. Unlike studies that focus only on people trying to quit, this one included all adult smokers. It found that people who vaped occasionally—meaning they used e-cigarettes on some days but not every day—were significantly (5.3%) less likely to quit smoking than those who didn’t vape. Importantly, people who vaped—whether daily or occasionally—were significantly less likely to be free from both smoking and vaping after four years. Compared to people who didn’t vape, those who vaped every day were 14.7% less likely and those who vaped occasionally were 7.2% less likely to quit nicotine entirely. This suggests that even when e-cigarettes help some people stop smoking, they may continue using nicotine by vaping instead.
Similarly, a 2020 study using data from the PATH cohort followed over 2,500 adult US smokers from 2014 to 2017 who reported trying to quit.15 It found no significant difference in long-term quit rates between those who used e-cigarettes and those who didn’t. However, approximately two-thirds of e-cigarette users who successfully quit smoking continued to vape, indicating that e-cigarettes may act as a substitute for smoking rather than help eliminate nicotine dependence.
In contrast, other studies suggest that vaping could increase the chances of quitting smoking. A 2022 study using data from the nationally representative PATH cohort followed over 10,000 adults aged 25 and older across multiple waves from 2013 to 2018 and found that e-cigarette users were more likely to quit smoking than non-users, even after adjusting for factors such as prior quit attempts and use of other tobacco products.16 However, the study did not differentiate between nicotine-containing and nicotine-free e-cigarettes.
A 2015 meta-analysis reviewed six studies involving over 7,500 participants from the US, UK, and Europe.17 It found that adults who used nicotine-containing e-cigarettes were more than twice as likely to quit smoking as those who used non-nicotine e-cigarettes. The authors also noted that many individuals who quit smoking continued using e-cigarettes, suggesting that e-cigarettes may serve as a substitute for cigarettes rather than a complete end to nicotine dependence.
A 2016 study reviewed 38 studies involving over 30,000 adults from the US, UK, and Europe—excluding PATH data—and found that people who used e-cigarettes were 28% less likely to quit smoking than those who did not use e-cigarettes.18 The analysis included 15 cohort studies, three cross-sectional studies, and two clinical trials. Among studies focusing on smokers actively trying to quit, e-cigarette users were 14% less likely to quit than non-users, although this difference was not statistically significant. The authors concluded that, as currently used, e-cigarettes are associated with reduced smoking cessation and should not be recommended as cessation aids without further evidence.
Given the results of these recent studies, why do so many people think vaping is a good way to quit smoking? Most of the early research on vaping and quitting were short term (six months or less), didn’t randomly assign smokers to different quit methods, and relied heavily on self-reported data. The better designed studies tended to show that vaping did not help people quit smoking. For example, a study conducted in four countries found that 85% of e-cigarette users said they were using them to quit smoking, yet they were no more likely to quit than regular smokers.19 A U.S. study published in 2014 found that although smokers often believed they were using e-cigarettes to quit, nearly all of them were still smoking regular cigarettes 6 to 12 months later.20 Similarly, a 2018 study found that 90% of smokers who used e-cigarettes were still smoking at the end of one year, even though they were more likely to say they were trying to quit.21
Although results vary, overall the studies show that vaping is not an effective way to quit smoking, and when smokers do quit, they are often replacing their smoking habit with a vaping habit, both of which involve addiction to nicotine.
Teenagers, Children, and Vaping
According to survey data collected between 2014 and 2017, 9% of middle and high schoolers reported that they were current vaping users. Vaping was most common among Native Hawaiian and Pacific Islanders (18%), as well as American Indian and Alaskan Native teens (13%). About 10% of White and Hispanic teens vaped, and vaping was least common among Black (5%) and Asian teens (4%).22 The percentage of teens who reported vaping doubled between 2017 and 2019.23 In 2019, about 28% of highschoolers and 11% of middle schoolers reported e-cigarette use. Most teens who vaped reported that they used flavored products.24 Two 2020 surveys found that the percentage of students vaping decreased early in the year. A CDC study analyzing data from the National Youth Tobacco Survey, a study of over 14,000 students, found that about 20% of 9th-12th grade students and 5% of 6th-8th grade students reported that they used e-cigarettes in the last 30 days.25 A different survey conducted by researchers from the University of Michigan, funded by the National Institute on Drug Abuse, studied over 8,000 students in only the 10th and 12th grades, and found that 22% reported vaping in the last 30 days.26 Although these numbers are still high, and comparable to the statistics in 2018,17 they are notably lower than 2019. E-cigarette use may have dropped due to growing awareness of the dangers of these products, including media coverage of young men hospitalized with serious lung damage.26,27 The drop may also be due to raising the legal age for the purchase of tobacco products and the ban on flavored products.27,28
It is important to note that these surveys conducted about e-cigarette use in 2020 were collected between January and March of 2020, and the surveys were stopped due to the COVID-19 pandemic.
An online survey conducted in May 2020 measured how e-cigarette use changed during the pandemic, during a time where many people are staying at home.29 The survey included almost 1,500 participants under 21 (the legal age to purchase tobacco products) who reported e-cigarette use. Over half of the underage e-cigarette users who responded to the survey reported that they had changed their e-cigarette use during the pandemic. About 20% of the sample had quit using e-cigarettes altogether, about 17% reduced their use slightly or by half, and another 9% actually increased their nicotine use.
The researchers followed up by asking those participants who reduced their e-cigarette use for the reasons why they lowered it. About 14% reported that the primary reason for reducing was because they were at home and their parents would know, 18% said the primary reason was because they can no longer get the tobacco products, 23% said it was because they know e-cigarette use harms the lungs, and another 37% said that their reasons were a combination of those 3 reasons. Of those who increased their use during the pandemic, about 25% reported that it was due to boredom, 15% because they were stressed, 7% because they needed a distraction, and about 50% said that their reasons were a combination of those 3 reasons.
Future research is needed to measure whether e-cigarette use has changed even more as the pandemic has continued, as well as to measure the overall percent of youth still using e-cigarettes.
E-cigarette and juul use by young people is worrisome for several reasons:
- The younger people are when they begin smoking, the more likely it is they will develop the habit: nearly 9 out of 10 smokers started before they were 18.30
- Nicotine and other chemicals found in e-cigarettes, juuls, etc. might harm brain development in younger people.31
- Vaping may introduce many more young people to smoking who might otherwise never have tried it, and once they are addicted to nicotine, some may decide to get their “fix” from regular cigarettes. Whether vaping or juuling is a “gateway” to regular cigarettes or not, young people who use them risk becoming addicted to nicotine and exposing their lungs to harmful chemicals.
- While smoking can cause permanent lung damage over the years, vaping can cause inflammation resulting in hospitalization and permanent damage after just a few weeks or months.32,33
The sharp rise in vaping among youth highlights the need to stop manufacturers from targeting teenagers with candy-like flavors and advertising campaigns. Although the FDA banned flavors for reusable vape devices, flavored disposable e-cigarettes are still being sold.20 However, in July 2020, FDA issued warnings to 10 companies selling flavored disposable e-cigarettes, notifying them to remove their products from the market because they do not have the authorizations required to sell them.34
Even children who are too young to smoke have been harmed by e-cigarettes and related products. The liquid is highly concentrated, so absorbing it through the skin or swallowing it is far more likely to require an emergency room visit than eating or swallowing regular cigarettes. In 2012, less than 50 kids under the age of six were reported to poison control hotlines per month because of e-cigarettes. In 2015, that number had skyrocketed to about 200 children a month, almost half of which were under the age of two!35
Many e-cigarettes look like USB devices, and some are made to look like other products, in order to disguise their use. The Director of Communications at the FDA’s Center for Tobacco Products has written this guide to help parents identify these hidden e-cigarettes. The FDA has also helped create this pamphlet for parents and teens to discuss the risks of vaping, and it provides resources for saying “no” and for quitting.
For more information about juuls, check out our article here.
How are these products regulated?
The FDA was given the power to regulate the manufacturing, labeling, distribution and marketing of all tobacco products in 2009 when President Obama signed into law the Family Smoking Prevention and Tobacco Control Act and in 2010 a court ruled that the FDA could regulate e-cigarettes as tobacco products.36

It wasn’t until 2016 that the FDA finalized a rule to regulate e-cigarettes, which would ban the sale of e-cigarettes to anyone under the age of 18 and would require all e-cigarettes that hit shelves after February 15, 2007 to go through a “premarket review,” the process that the FDA uses to determine whether potentially risky products are safe.26 Companies were to be given from 18 months to two years to comply with this rule and prepare their applications. However, in 2017, the Trump administration appointed a new FDA Commissioner, Dr. Scott Gottlieb, who defended the safety of e-cigarettes and delayed implementing the rules until 2022.9 Nevertheless, as the epidemic of e-cigarette use among youth became obvious, in 2018, Commissioner Gottlieb threatened to crack down on the advertising of e-cigarettes to children under 18.37 Critics have questioned whether sales and ads can be effectively restricted. Moreover, Commissioner Gottlieb resigned in 2019, and it is unclear how the agency will respond to the growing evidence that vaping can cause serious harm. However, in 2019, a federal court ruled that the FDA must implement regulations in May 2020 instead of waiting until 2022.
In September, President Trump responded to the health crisis by proposing a ban on flavored e-cigarettes. Two months later, the administration has not taken any action as Trump states that he is worried children will seek out unsafe alternatives if flavors are banned. In the meantime, individual states have always had the power to pass laws restricting the sale and use of e-cigarettes. Current laws pertaining to e-cigarettes are available on the Public Health Law Center website.
The Bottom Line
E-cigarettes, juuls, and other similar products have not been around long enough to determine the harm they cause in the long run. Unfortunately, many people, including teenagers, are under the impression that e-cigarettes are safe or that they are effective in helping people quit smoking regular cigarettes. Studies by the FDA show that e-cigarettes contain some of the same toxic chemicals as regular cigarettes, even though they don’t have tobacco. There is evidence that some of these toxic chemicals can cause DNA damage that can cause cancer. More important, the reports of teens and adults who died or were hospitalized due to vaping are proof that vaping can be extremely dangerous even after just a few weeks, months, or years.
The big three tobacco companies—Lorillard, Reynolds American, and Altria Group—all have their own e-cigarette brands, so it’s not surprising that e-cigarettes are being marketed and advertised much the way regular cigarettes used to be. Here are the 7 Ways E-Cigarette Companies Are Copying Big Tobacco’s Playbook.
Although there are clearly serious dangers from vaping, more research is needed to confirm the impact of vaping on DNA damage, especially in children. Meanwhile, claims that e-cigarettes are an effective strategy to quit smoking are not supported by the evidence thus far. In addition, more toxicological studies and epidemiological studies are needed to understand the hundreds of reports of permanent lung damage and deaths from vaping. It is essential to find out whether some types of vaping are more dangerous than others in the short-term and the long-term. To understand the risks for everyone who vapes, research is needed to compare the risks of specific brands of e-cigarettes with tobacco products, as well as to neither smoking nor vaping.
All articles are reviewed and approved by Dr. Diana Zuckerman and other senior staff.
The National Center for Health Research is a nonprofit, nonpartisan research, education and advocacy organization that analyzes and explains the latest medical research and speaks out on policies and programs. We do not accept funding from pharmaceutical companies or medical device manufacturers. Find out how you can support us here.
- Robert Langreth. More Evidence Links Vaping Lung Injuries to Vitamin E Acetate. December 20, 2019.
https://www.bloomberg.com/news/articles/2019-12-20/more-evidence-links-vaping-lung-injuries-to-vitamin-e-acetate
- Centers for Disease Control and Prevention. Outbreak of Lung Injury Associated with the Use of E-Cigarette, or Vaping, Products. Updated 2020. https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html
- O’Connor RJ. Non-cigarette tobacco products: What have we learned and where are we headed? Tobacco Control. 2012;21(2): 181–190. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3716250/
- Gaiha SM, Cheng J, Halpern-Felsher B. Association between youth smoking, electronic cigarette use, and COVID-19. Journal of Adolescent Health. 2020;67(4):519-523. doi:10.1016/j.jadohealth.2020.07.002
- Food and Drug Administration. Summary of Results: Laboratory analysis of electronic cigarettes conducted By FDA. FDA News & Events. July 22 2009.
- Varlet V, Farsalinos K, Augsburger M, et al. Toxicity of refill liquids for electronic cigarettes. International Journal for Environmental Research and Public Health. 2015;12:4796-4815. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4454939/
- Pankow JF, Kim K, McWhirter KJ, et al. Benzene formation in electronic cigarettes. PLOS ONE. 2017;12(3),e0173055. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/28273096/
- Centers for Disease Control and Prevention. Overviews of Diseases/Conditions. February 2019. https://www.cdc.gov/tobacco/campaign/tips/diseases/index.html
- McGinley, L. FDA sued for delaying e-cigarette, cigar regulations. Washington Post. March 27 2018. https://www.washingtonpost.com/news/to-your-health/wp/2018/03/27/fda-sued-for-delaying-e-cigarette-cigar-regulations/?utm_term=.f92695720619.
- Lee HW, Park SH, Weng MW, et al. E-cigarette smoke damages DNA and reduces repair activity in mouse lung, heart, and bladder as well as in human lung and bladder cells. Proceedings of the National Academy of Sciences of the United States of America. 2018;115(7), E1569. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5816191/
- Kaisar MA, Prasad S, Liles T, et al. A decade of e-cigarettes: Limited research & unresolved safety concerns. Toxicology. 2016;365: 67–75. http://doi.org/10.1016/j.tox.2016.07.020
- Robert Langreth. More Evidence Links Vaping Lung Injuries to Vitamin E Acetate. December 20, 2019.
https://www.bloomberg.com/news/articles/2019-12-20/more-evidence-links-vaping-lung-injuries-to-vitamin-e-acetate
- Kaplan S. E-Cigarette exploded in a teenager’s mouth, damaging his jaw. The New York Times. June 19 2019. https://www.nytimes.com/2019/06/19/health/ecigarettes-explosion.html
- Quach, N. E., Pierce, J. P., Chen, J., Dang, B., Stone, M. D., Strong, D. R., Trinidad, D. R., McMenamin, S. B., & Messer, K. (2025). Daily or Nondaily Vaping and Smoking Cessation Among Smokers. JAMA network open, 8(3), e250089. https://doi.org/10.1001/jamanetworkopen.2025.0089
- Chen, R., Pierce, J. P., Leas, E. C., White, M. M., Kealey, S., Strong, D. R., Trinidad, D. R., Benmarhnia, T., & Messer, K. (2020). Use of Electronic Cigarettes to Aid Long-Term Smoking Cessation in the United States: Prospective Evidence From the PATH Cohort Study. American journal of epidemiology, 189(12), 1529–1537. https://doi.org/10.1093/aje/kwaa161
- Lee, P. N., & Fry, J. S. (2020). Investigating the effect of e-cigarette use on quitting smoking in adults aged 25 years or more using the PATH study. F1000Research, 9, 1099. https://doi.org/10.12688/f1000research.26167.3
- Rahman, M. A., Hann, N., Wilson, A., Mnatzaganian, G., & Worrall-Carter, L. (2015). E-cigarettes and smoking cessation: evidence from a systematic review and meta-analysis. PloS one, 10(3), e0122544. https://doi.org/10.1371/journal.pone.0122544
- Kalkhoran, S., & Glantz, S. A. (2016). E-cigarettes and smoking cessation in real-world and clinical settings: a systematic review and meta-analysis. 18The Lancet. Respiratory medicine, 4(2), 116–128. https://doi.org/10.1016/S2213-2600(15)00521-4
- Adkison SE, O’Connor RJ, Bansal-Travers M, et al. Electronic nicotine delivery systems: International tobacco control four-country survey. American Journal of Preventive Medicine. 2013;44(3):207-215. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/23415116/
- Grana RA, Popova L, Ling PM. A longitudinal analysis of electronic cigarette use and smoking cessation. JAMA Internal Medicine. 2014;174(5):812–813. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4122246/
- Food and Drug Administration. Electronic Cigarettes. FDA News & Events. 25 July 2013.
- Odani S, Armour BS, Agaku IT. Racial/ethnic disparities in tobacco product use among middle and high school students—United States, 2014–2017. Morbidity and Mortality Weekly Report. 2018 Aug 31;67(34):952.
- Miech R, Johnston L, O’Malley PM, Bachman JG, Patrick ME. Trends in adolescent vaping, 2017–2019. New England Journal of Medicine. 2019 Oct 10;381(15):1490-1.
- Cullen KA, Gentzke AS, Sawdey MD, Chang JT, Anic GM, Wang TW, Creamer MR, Jamal A, Ambrose BK, King BA. E-cigarette use among youth in the United States, 2019. JAMA. 2019 Dec 3;322(21):2095-103.
- Gentzke AS, Wang TW, Jamal A, et al. Tobacco Product Use Among Middle and High School Students — United States, 2020. MMWR Morb Mortal Wkly Rep 2020;69:1881–1888. DOI: http://dx.doi.org/10.15585/mmwr.mm6950a1external icon.
- Miech R, Leventhal A, Johnston L, O’Malley PM, Patrick ME, Barrington-Trimis J. Trends in Use and Perceptions of Nicotine Vaping Among US Youth From 2017 to 2020. JAMA Pediatrics. Published online December 15, 2020. doi:10.1001/jamapediatrics.2020.5667
- Grady D. A Young Man Nearly Lost His Life to Vaping. The New York Times. October 15, 2019. https://www.nytimes.com/2019/10/15/health/vaping-thc-illness.html
- Stobbe S, Perrone M. Big drop reported in vaping by US teenagers. Associated Press. September 9, 2020. https://apnews.com/c5524d4c1e7f9148c3293cc3677c0fe5
- Gaiha SM, Lempert LK, Halpern-Felsher B. Underage Youth and Young Adult e-Cigarette Use and Access Before and During the Coronavirus Disease 2019 Pandemic. JAMA Network Open. 2020 Dec 1;3(12):e2027572-.
- Centers for Disease Control and Prevention. Fact sheets: Youth and tobacco use. Updated 2019. http://www.cdc.gov/tobacco/data_statistics/fact_sheets/youth_data/tobacco_use/
- Centers for Disease Control and Prevention. Preventing tobacco use among youth and young adults. 2012. http://www.cdc.gov/tobacco/data_statistics/sgr/2012/index.htm
- Scutti S. Teen develops ‘wet lung’ after vaping for just 3 weeks. CNN. May 18, 2018. https://www.cnn.com/2018/05/17/health/case-study-teen-vaping-wet-lung/index.html
- Song MA, Reisinger SA, Freudenheim JL, Brasky TM, Mathé EA, McElroy JP, Nickerson QA, Weng DY, Wewers MD, Shields PG. Effects of electronic cigarette constituents on the human lung: A pilot clinical trial. Cancer Prevention Research. 2020 Feb 1;13(2):145-52.
- U.S. Food and Drug Administration. FDA Notifies Companies, Including Puff Bar, to Remove Flavored Disposable E-Cigarettes and Youth-Appealing E-Liquids from Market for Not Having Required Authorization. Updated July 2020. https://www.fda.gov/news-events/press-announcements/fda-notifies-companies-including-puff-bar-remove-flavored-disposable-e-cigarettes-and-youth
- Kamboj A, Spiller HA, Casavant MJ, et al. Pediatric exposure to e-cigarettes, nicotine, and tobacco products in the United States. Pediatrics. 2016;137(6). pii: e20160041. https://pediatrics.aappublications.org/content/137/6/e20160041.long
- Food and Drug Administration. Regulation of E-Cigarettes and Other Tobacco Products. FDA News & Events. April 25, 2011.
- Saltzman J, Freyer F. The FDA issues a warning: Teen vaping is ‘an epidemic.’ Boston Globe. September 13 2018. https://www.bostonglobe.com/metro/2018/09/12/fda-cracks-down-vaping-orders-makers-address-sales-minors/JaiqQYzZAl4CINLufnkKlL/story.html



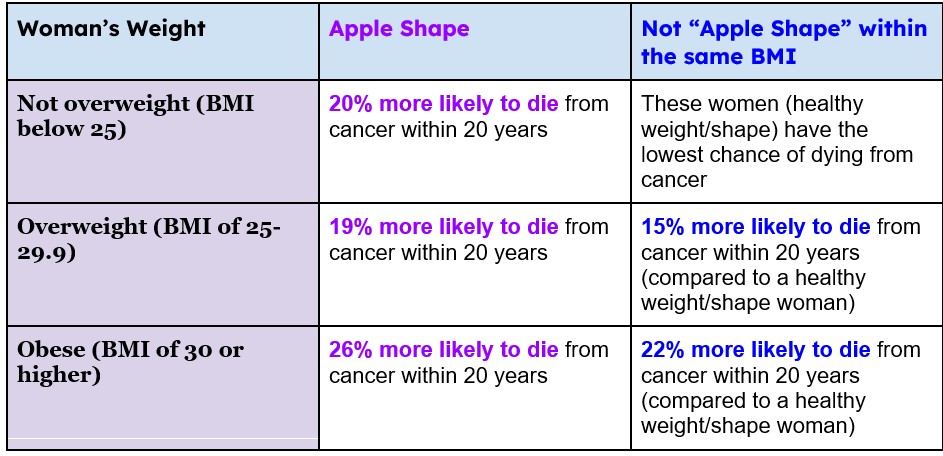 Table 2. Likelihood of death due to cancer in women based on BMI. 3
Table 2. Likelihood of death due to cancer in women based on BMI. 3