
Farmin Shahabuddin, MPH, Cancer Prevention and Treatment Fund
Most people know that exercise is good for your heart and overall health. What many people do not know is that exercise may also reduce the likelihood of developing cancer and help cancer survivors live longer after treatment ends. Whether you have never had cancer or finished treatment and want to lower your chances of it coming back, physical activity is one of the most important things you can do.
Can Exercise Reduce Your Likelihood of Getting Cancer?
Research shows that people who are physically active are less likely to develop many types of cancer. A study of 1.4 million people found that those who exercised regularly were less likely to develop 13 types of cancer, including breast, colon, liver, kidney, stomach, and bladder cancer.1
A 2025 study tracked activity of more than 85,000 adults using wearable devices. The most active people were about 26% less likely to develop cancer than the least active.2 Even light activities such as errands and household chores made a difference. Taking more steps each day also helped. For example, people who took 9,000 steps a day were about 16% less likely to develop cancer than those who took 5,000.
Cancer usually is growing before it is diagnosed, and being active in the year before a diagnosis is also beneficial according to a 2025 study of more than 28,000 people with stage 1 cancers who had activity records for the year before their diagnosis.3 Those who exercised as little as 60 minutes per week were 27% less likely to have their cancer progress to a more advanced stage and were 47% less likely to die, compared to those who were not active.3 Five years after diagnosis, about 91% of the most active people were still alive, compared to about 84% of those who had not been active.3
Why Does Exercise Lower the Likelihood of Cancer?
Exercise may lower the likelihood of cancer in several ways. It lowers hormones such as estrogen and insulin that can encourage cancer cells to grow.4,5,6 It helps the immune system spot and destroy abnormal cells.6 It also helps people maintain a healthy weight, which matters because being overweight contributes to an estimated 14% to 20% of cancer deaths in the U.S.6 Exercise also helps move food through the digestive system faster, which reduces the time that the lining of the intestines is exposed to potentially harmful substances.
Scientists are still learning more about why exercise can prevent cancer. A 2026 lab study found that even 10 minutes of exercise changed the blood in ways that helped colon cancer cells repair damaged DNA.7 While more research is needed, this adds to the evidence that exercise sends signals throughout the body that may help fight cancer.
How Much Exercise Do You Need?
The U.S Department of Health and Human Services physical activity guidelines recommend that all adults get 150 to 300 minutes per week of moderate activity such as brisk walking, or 75 to 150 minutes of vigorous activity such as running. Adults should also do muscle strengthening exercises at least 2 days per week.6 These guidelines are not specific to cancer prevention. Of course, any amount of physical activity is better than none. The key is to start where you are and gradually build up.
Exercise for Cancer Survivors After Treatment
Exercise does not just matter before a cancer diagnosis. It can also be helpful during cancer treatment (see this link for our article on that). Regular exercise after you have finished cancer treatment, can also help you live longer and feel better, with fewer side effects from treatment, including less fatigue.8,9 Survivors who exercise regularly are less likely to die from cancer and are more likely to live longer than those who do not exercise.[10-14] It does not matter if you were fit before you got diagnosed. What matters is that you start exercising now.
Since exercise improves the immune system, cancer survivors who exercise regularly lower their chances of the cancer returning. A large 2026 study followed more than 17,000 cancer survivors for an average of about 11 years. 15 The survivors had bladder, endometrial, lung, oral cavity, ovarian, or rectal cancer. The activities studied included brisk walking, cycling, and swimming. The study compared survivors at different activity levels to those who did no physical activity at all. It found that even small amounts of exercise that were considerably less than the recommended physical activity guidelines, were linked to longer survival. Bladder cancer survivors who did relatively low levels of exercise were 33% less likely to die from their cancer, endometrial cancer survivors were 38% less likely, and lung cancer survivors were 44% less likely, compared to those who did no physical activity.
Survivors who met or exceeded the recommended guidelines saw even greater benefits. Endometrial cancer survivors who met the guidelines were 60% less likely to die from their cancer, and lung cancer survivors were 62% less likely, compared to those who did no exercise. Oral and rectal cancer survivors who doubled the recommended amount of activity were 61% less likely to die of oral cancer and 43% less likely to die of rectal cancer.
Sitting Less Matters Too
Along with exercising more, sitting less can also make a difference. A 2022 study followed over 1,500 cancer survivors ages 40 and over for an average of 4.5 years. Survivors who exercised at least 150 minutes per week were less likely to die than those who did not exercise. 16 Survivors who sat for more than 8 hours a day were also more likely to die than those who sat less than 4 hours per day. Those who both did not exercise and sat more than 8 hours per day had the worst outcomes of all.”
A 2020 study followed 8,000 adults aged 45 and older for about 5 years. People who sat the most were more likely to die from cancer than those who sat the least.17 Replacing just 30 minutes of sitting per day with moderate to vigorous activity was linked to a 31% lower chance of dying from cancer. Even replacing that sitting time with light activity like standing or gentle walking was linked to an 8% lower chance of dying.
What Kind of Exercise Should I Do?
Aerobic activity of light to moderate intensity was the most common type of exercise studied in cancer patients. Combining aerobic exercise with walking and resistance training, such as lifting weights or resistance bands, led to greater health benefits than aerobic activity alone.11,13 Lifting weights refers to any weights, even just a few pounds. Do not assume you need barbells and large muscles.
Walking is the easiest way to start. The greatest benefit comes from walking at an average speed, about a 20-minute mile, for 3 to 5 hours per week.8 Even walking just 1 hour per week showed improvements over no physical activity at all.
The most important thing is to make it a habit. Start small by taking the stairs instead of the elevator or walking after dinner each evening. It is better to start small and keep it up than to try to do too much and give up. Do not miss the chance to get at least some benefit from this easy, free way to fight cancer.
The Bottom Line
Exercise is a powerful, free tool. For people who have never had cancer, regular physical activity is linked to a lower likelihood of developing many types of cancer. For survivors who have finished treatment, exercise lowers the chances of cancer coming back and helps people live longer. Being active before a diagnosis also improves outcomes if cancer does occur. Even if you were not active before, starting to exercise afterward still helps. Try to walk 3 to 5 hours a week at an average pace, about 1 mile per 20 minutes. Try to sit less and move more throughout the day. Even a little exercise is better than none. It is never too late to begin.
To read about the benefits of exercise during cancer treatment, click here: https://stopcancerfund.org/pz-diet-habits-behaviors/exercise-cancer-treatment-benefits/
References
- Moore, S. C., Lee, I. M., Weiderpass, E., Campbell, P. T., Sampson, J. N., Kitahara, C. M., Keadle, S. K., Arem, H., Berrington de Gonzalez, A., Hartge, P., Adami, H. O., Blair, C. K., Borch, K. B., Boyd, E., Check, D. P., Fournier, A., Freedman, N. D., Gunter, M., Johansson, M., & Patel, A. V. (2016). Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. JAMA Internal Medicine, 176(6), 816–825. https://doi.org/10.1001/jamainternmed.2016.1548
- National Cancer Institute. (2025, March 26). Cancer risk decreases with more physical activity [Press release]. https://www.cancer.gov/news-events/press-releases/2025/light-intensity-physical-activity-cancer-risk
- Patricios, J., Constantinou, D., Goff, P., Kolbe-Alexander, T., Capostagno, B., Gossage, S., & van Rensburg, D. C. J. (2025). Regular physical activity before cancer diagnosis may lower progression and death risks. British Journal of Sports Medicine. https://doi.org/10.1136/bjsports-2024-108699
- Key, T., Appleby, P., Barnes, I., & Reeves, G. (2002). Endogenous sex hormones and breast cancer in postmenopausal women: Reanalysis of nine prospective studies. Journal of the National Cancer Institute, 94(8), 606–616. https://doi.org/10.1093/jnci/94.8.606
- McTiernan, A., Tworoger, S. S., Ulrich, C. M., Yasui, Y., Irwin, M. L., Rajan, K. B., Sorensen, B., Rudolph, R. E., Bowen, D., Stanczyk, F. Z., Potter, J. D., & Schwartz, R. S. (2004). Effect of exercise on serum estrogens in postmenopausal women: A 12-month randomized clinical trial. Cancer Research, 64(8), 2923–2928. https://doi.org/10.1158/0008-5472.CAN-03-3393
- National Cancer Institute. (n.d.). Physical activity and cancer fact sheet. U.S. Department of Health and Human Services. https://www.cancer.gov/about-cancer/causes-prevention/risk/obesity/physical-activity-fact-sheet
- Orange, S. T., Dodd, E., Nath, S., Bowden, H., Jordan, A. R., Tweddle, H., Hedley, A., Chukwuma, I., Hickson, I., & Sharma Saha, S. (2025). Exercise serum promotes DNA damage repair and remodels gene expression in colon cancer cells. International Journal of Cancer. https://doi.org/10.1002/ijc.70271
- Holmes, M. D., Chen, W. Y., Feskanich, D., Kroenke, C. H., & Colditz, G. A. (2005). Physical activity and survival after breast cancer diagnosis. JAMA, 293(20), 2479–2486. https://doi.org/10.1001/jama.293.20.2479
- McNeely, M. L., Campbell, K. L., Rowe, B. H., Klassen, T. P., Mackey, J. R., & Courneya, K. S. (2006). Effects of exercise on breast cancer patients and survivors: A systematic review and meta-analysis. Canadian Medical Association Journal, 175(1), 34–41. https://doi.org/10.1503/cmaj.051073
- Meyerhardt, J. A., Heseltine, D., Niedzwiecki, D., Hollis, D., Saltz, L. B., Mayer, R. J., Thomas, J., Nelson, H., Whittom, R., Hantel, A., Schilsky, R. L., & Fuchs, C. S. (2006). Impact of physical activity on cancer recurrence and survival in patients with stage III colon cancer: Findings from CALGB 89803. Journal of Clinical Oncology, 24(22), 3535–3541. https://doi.org/10.1200/JCO.2006.06.0863
- Fong, D. Y. T., Ho, J. W. C., Hui, B. P. H., Lee, A. M., Macfarlane, D. J., Leung, S. S. K., Cerin, E., Chan, W. Y. Y., Leung, I. P. F., Lam, S. H. S., Taylor, A. J., & Cheng, K. K. (2012). Physical activity for cancer survivors: Meta-analysis of randomized controlled trials. BMJ, 344, e70. https://doi.org/10.1136/bmj.e70
- Meyerhardt, J. A., Giovannucci, E. L., Holmes, M. D., Chan, A. T., Chan, J. A., Colditz, G. A., & Fuchs, C. S. (2006). Physical activity and survival after colorectal cancer diagnosis. Journal of Clinical Oncology, 24(22), 3527–3534. https://doi.org/10.1200/JCO.2006.06.0855
- Spence, R. R., Heesch, K. C., & Brown, W. J. (2010). Exercise and cancer rehabilitation: A systematic review. Cancer Treatment Reviews, 36(2), 185–194. https://doi.org/10.1016/j.ctrv.2009.11.003
- Sternfeld, B., Weltzien, E., Quesenberry, C. P., Jr., Castillo, A. L., Kwan, M., Slattery, M. L., & Caan, B. J. (2009). Physical activity and risk of recurrence and mortality in breast cancer survivors: Findings from the LACE study. Cancer Epidemiology, Biomarkers & Prevention, 18(1), 87–95. https://doi.org/10.1158/1055-9965.EPI-08-0595
- Rees-Punia, E., Teras, L. R., Newton, C. C., Gapstur, S. M., Patel, A. V., Gaudet, M. M., Islami, F., Campbell, P. T., & McCullough, M. L. (2026). Leisure-time physical activity and cancer mortality among cancer survivors. JAMA Network Open, 9(2), e2556971. https://doi.org/10.1001/jamanetworkopen.2025.56971
- Cao, C., Friedenreich, C. M., & Yang, L. (2022). Association of daily sitting time and leisure-time physical activity with survival among US cancer survivors. JAMA Oncology, 8(3), 395–403. https://doi.org/10.1001/jamaoncol.2021.6590
- Gilchrist, S. C., Howard, V. J., Akinyemiju, T., Judd, S. E., Cushman, M., Hooker, S. P., & Diaz, K. M. (2020). Association of sedentary behavior with cancer mortality in middle-aged and older US adults. JAMA Oncology, 6(8), 1210–1217. https://doi.org/10.1001/jamaoncol.2020.2045


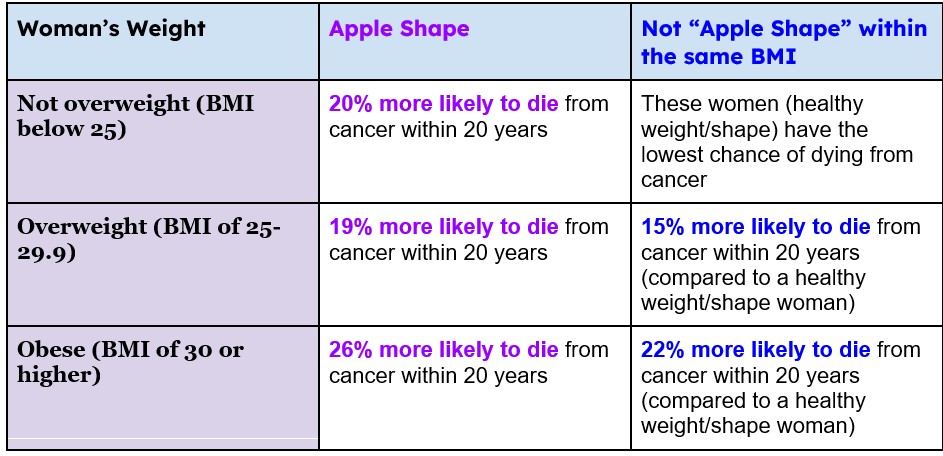 Table 2. Likelihood of death due to cancer in women based on BMI. 3
Table 2. Likelihood of death due to cancer in women based on BMI. 3
