
Diana Zuckerman, PhD, Cancer Prevention & Treatment Fund
Most of us know cancer patients who received drugs that drained their energy and joy of living but didn’t seem to benefit them. In some cases, the cancer stopped growing within a few months and even began to shrink, but ultimately the patient did not seem to live even a day longer.
Why is that?
A key problem is that cancer drugs do not have to be proven to prolong anyone’s life in order for the Food and Drug Administration (FDA) to approve them. Researchers at the National Cancer Institute and Oregon Health & Science University reviewed all the cancer drugs approved by the FDA from 2008 to 2012 (Kim & Prasad). They found that 26 of the 54 cancer drugs were not required to be proven to prolong or save lives, but instead were approved based on what are called surrogate markers, which are “signs” such as tumor shrinkage that are expected (but not guaranteed) to predict patients’ longer life.
Once the drugs were approved, thousands of patients started taking these drugs and paying for them, despite the lack of evidence of a meaningful health benefit. However, the FDA did require the companies to keep studying the drugs to find out if those medicines were actually extending lives.
The answer, unfortunately, is that many of these drugs did not help patients live longer or better. Only five of the 36 drugs were proven to help patients live longer. Eighteen drugs (50%) failed to extend life and 13 (36%) have unknown impact on survival because no data on them are available to the public. Since companies are very good at sharing information when their drugs are proven effective, experts assume that means those 13 drugs are not proven to work.
In November 2016, the National Center for Health Research published a study looking more carefully at those 18 ineffective drugs. We found that only one was proven to improve quality of life – which isn’t surprising, since cancer drugs so often cause nausea, vomiting, hair loss, and exhaustion. Two made quality of life worse, and the other 15 new cancer drugs either did not improve quality of life (6), or there is not enough evidence to know if they do or not. We also looked at the cost of those cancer drugs and found something that doctors, patients, family members, and lawmakers need to know: the new cancer drugs that are not proven to benefit patients in any way cost just as much as the ones that are effective – up to $170,000 per patient. In fact, the most expensive of the 18 cancer drugs was a thyroid cancer drug (Cabozantinib, also called Cabometyx or Cometriq) that had no benefit to survival compared to placebo, and also caused patients to have a worse quality of life.
Meanwhile, the ineffective cancer drugs remain on the market and Medicare and insurers are still paying for them. When the president of the National Center for Health Research asked FDA officials why they take so long to rescind the approval of ineffective cancer drugs, they stated that they still think those drugs might be effective, but that it is difficult to prove. They pointed out that once a cancer drug is approved, it is very difficult to keep patients in a clinical trial long enough to know if the drug actually saves lives. We agree it is difficult; if a patient is in a clinical trial and not doing well, he or she is likely to drop out, whether they are on the new drug, old drug, or placebo. But that’s a major problem: if the FDA is approving cancer drugs on short-term, inconclusive data, and then requiring better studies that they know are unlikely to be completed appropriately, that’s quite a Catch-22. It means that the FDA is approving cancer drugs knowing that we’ll never know if they are safe and effective or not.
This article is based on this study in JAMA Internal Medicine.1
Table 1. Most New Cancer Drugs That Don’t Help Patients Live Longer Also Don’t Improve Their Quality of Life
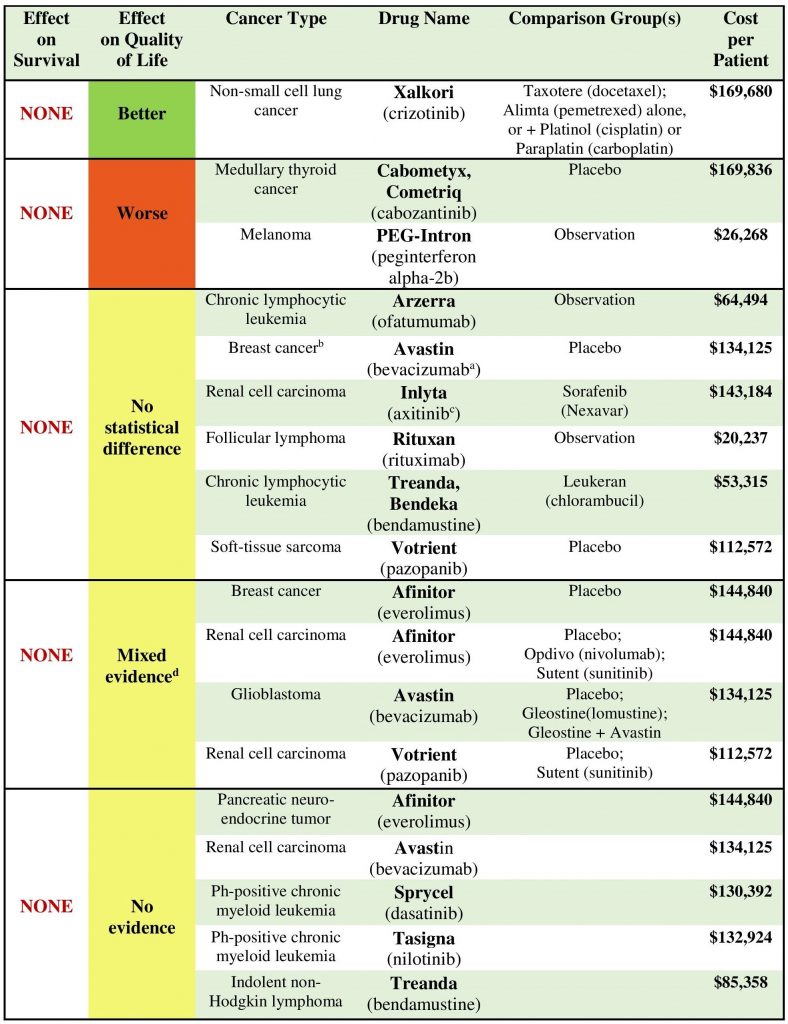
a FDA review notes that sponsor stated one study found a difference in deterioration of QoL that was statistically significant in favor of bevacizumab.
b On November 18, 2011, FDA revoked accelerated approval of the breast cancer indication for bevacizumab.
c One subgroup analysis of Japanese patients found a QoL benefit.
d Includes any combination of the other categories (better, no statistical difference, worse).
P.S. In 2019, cancer therapy drug Lartruvo failed to meet the main goal in a late-stage trial testing the therapy in patients with advanced or metastatic soft tissue sarcoma. Read more here.
- Rupp T, Zuckerman D. Quality of Life, Overall Survival, and Costs of Cancer Drugs Approved Based on Surrogate Endpoints. JAMA Intern Med. Published online November 29, 2016. doi:10.1001/jamainternmed.2016.7761 ▲